Tomorrow, would be our last day into the next extension of our enhanced community quarantine (ECQ), otherwise called a lockdown.
While I try to make sense of the numerical values that are being provided by the government, one cannot help but be skeptical about the kind of information that is being gathered.
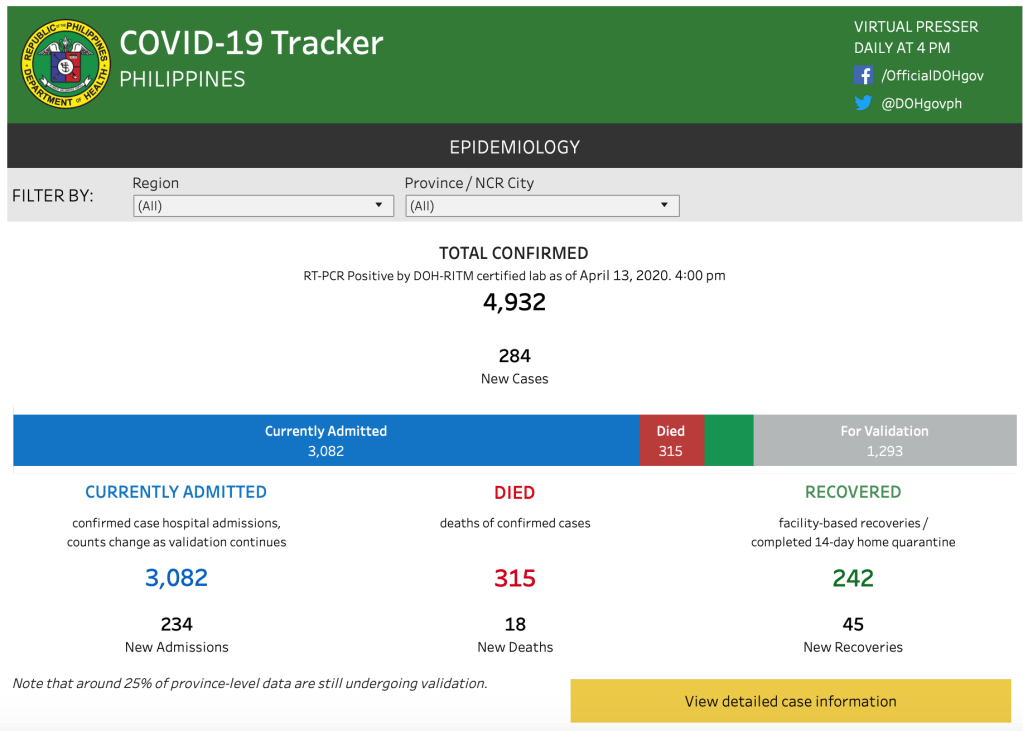
During one of the online meetings, the easiest question asked was – “what do I make of the numbers” that are being announced daily regarding the aCOVID-19 statistics?
After all, it’s been 45 days since the lockdown.
The anatomy of disappointment are expectations.
We expect that the government has and is doing enough at addressing the pandemic in the Philippines. Although we know that politics plays a role in how this pandemic is addressed, I will not delve into this. (But I would still caution any government or anyone for that matter that utilizes politics as a means for future political mileage to check their moral compass.) After all, no one will ever be prepared for a crisis of this magnitude. No government will have concrete immediate answers to the crisis at hand. All they can do now, is try the very best to approach this issue in a scientific, sensible, feasible, realizable, rational manner.
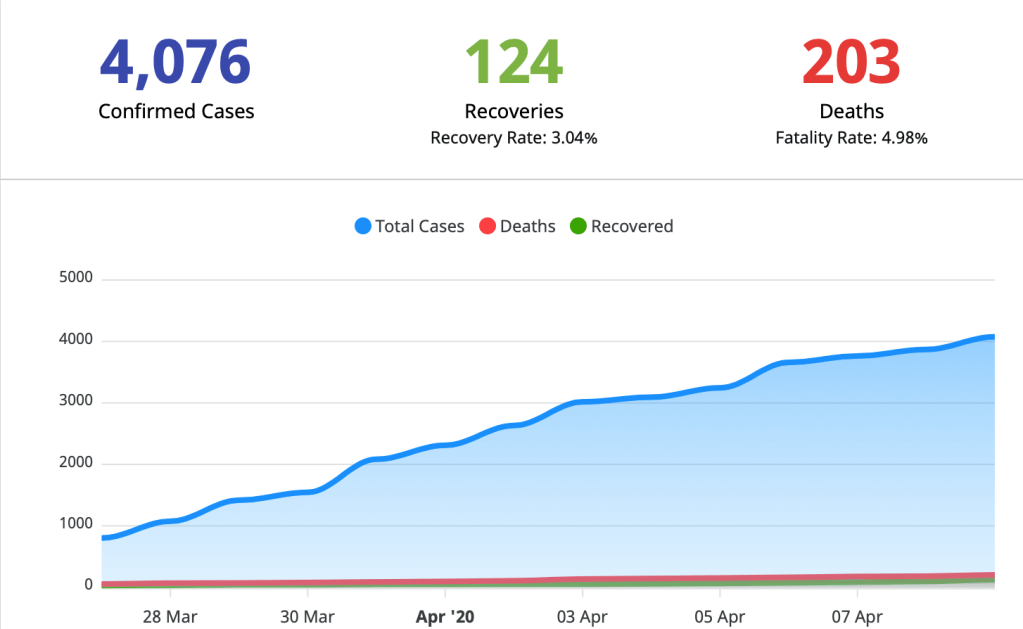
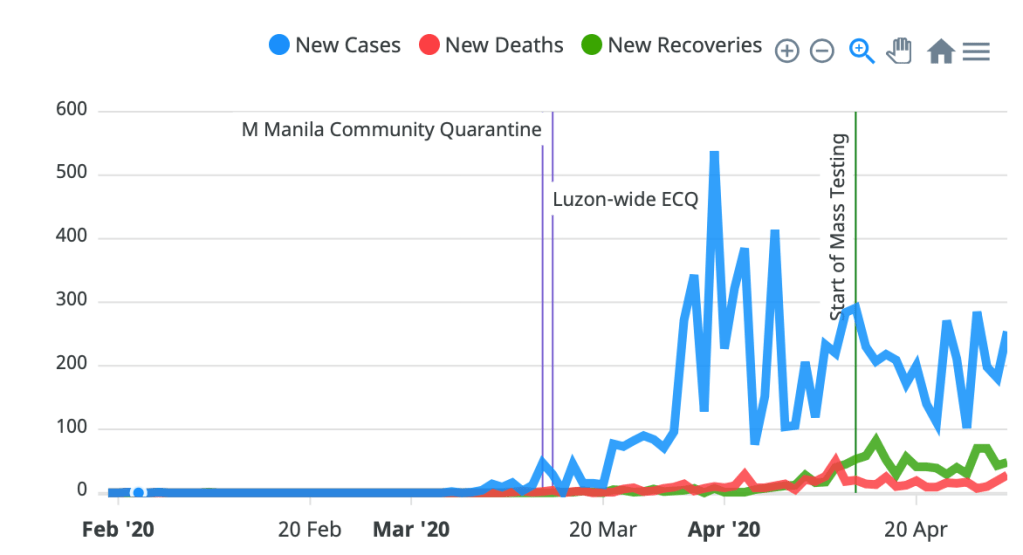
I am sure most of us were expecting that with the initial 30 days ECQ, the number of cases – admission and deaths – would have gone down, and see more recoveries. But the first 30 days simply showed dismal numbers. Plotted on a linear graph, Figure 1 below shows the see-saw of daily data being reported.
So we go back to the question asked. How do you interpret this data?
The answer is simple. With caution.
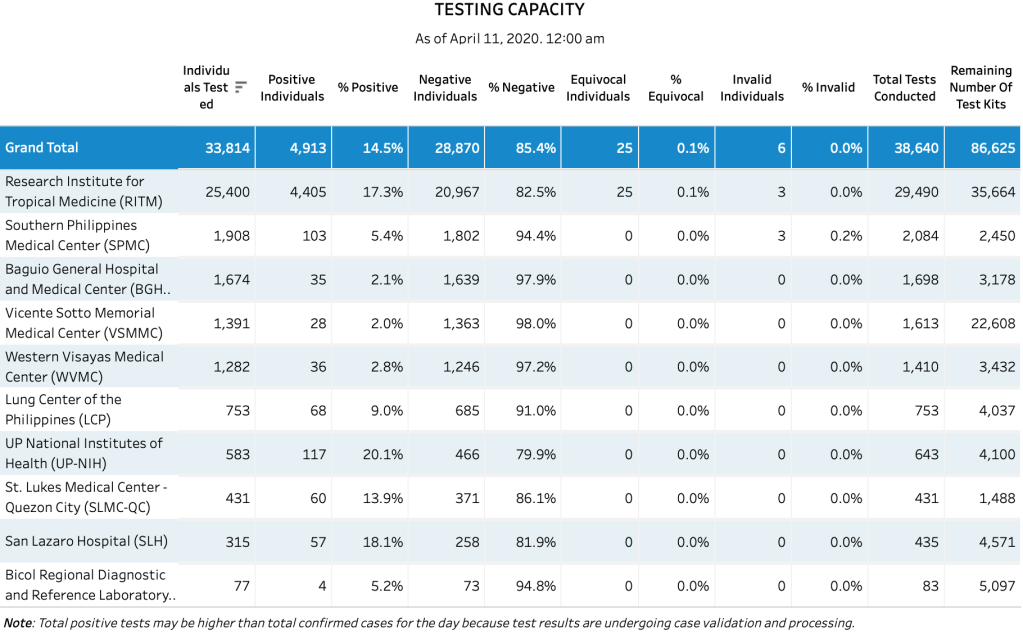
The numbers that come in are just numerical values. Considering the various constraints the Department of Health is encountering in the transmittal, accuracy of information being given to them from the various local government units, and verification of data – it is difficult to make heads or tails with the numbers. These factors account for latency in data. Many people look at the numbers and jump to the conclusion that we have too many deaths and too few recoveries. A quick look at daily data being churned out makes one presume that all these may have happened “the day before”.
On the other hand, if I converted the graph to a logarithmic scale, the data of the Philippines would look like what we have in figure 2. Instead of the see-saw pattern, you’d get a curve.

A logarithmic scale is very different from a linear one. In short, a logarithmic scale best expresses the exponential growth of what we want to measure. In this case on Figure 2, the total confirmed COVID-19 cases and how rapidly they are increasing.
The logarithmic scale can only be plotted once the first 100 patients are reached (so that we can measure exponential growth). The Philippines reached that on March 15, 2020 with 111 confirmed cases. The X-axis shows the cases over time (number of days since the 100th confirmed case). The light grey colored lines at the background show where we are in terms of doubling time based on the data we have. Twenty (20) days after our first 100th confirmed case, our doubling time was approximately 3-5 days (~4.2) with 3,870 confirmed cases around April 4. Forty days after our first 100th confirmed case, our doubling time is now between 5-10 (~7.5) with 8212 total confirmed cases to date.
Which means, we’re now bending the curve because the growth rate has markedly decline to an average of 2.8%.
But all these data have no meaning when you take into consideration the inaccuracy due to reporting errors and problems seen on the ground.
Why do we need to be obsessed with data accuracy?
It’s a simple answer.
The decisions being made for and on behalf of this crisis hinges on quality data. Any decision for that matter cannot be drawn from gut feeling. Decisions and recommendations made need to make recommendations backed up by solid data that will withstand scrutiny. While there will be acceptable gaps, these gaps when recognized early on should be addressed immediately because the extension of the ECQ was primarily based on the issue of not being able to “flatten the curve” or in this case, bending the curve.
The second important parameter will always be death.
Deaths (more than recoveries) provide closure to any event. Looking at the curve for death from an overall number of cases (see Figure 1) may give us a false sense of security. One glance and one can see that on a linear scale, our deaths are but a handful each day. But the latency in death reports in the Philippines average ~6.5 days, with more than 35% being reported after 8 days or more. As of yesterday, 316 of the deaths were reported posthumously – they died before they were even declared positive from the virus.
The quality of these numbers is disappointing because the other ramifications of good contact tracing, isolation and quarantine and work-up of patients exposed to those that have had the disease becomes a work nightmare and is hazardous to healthcare workers who are falling off the grid like flies.
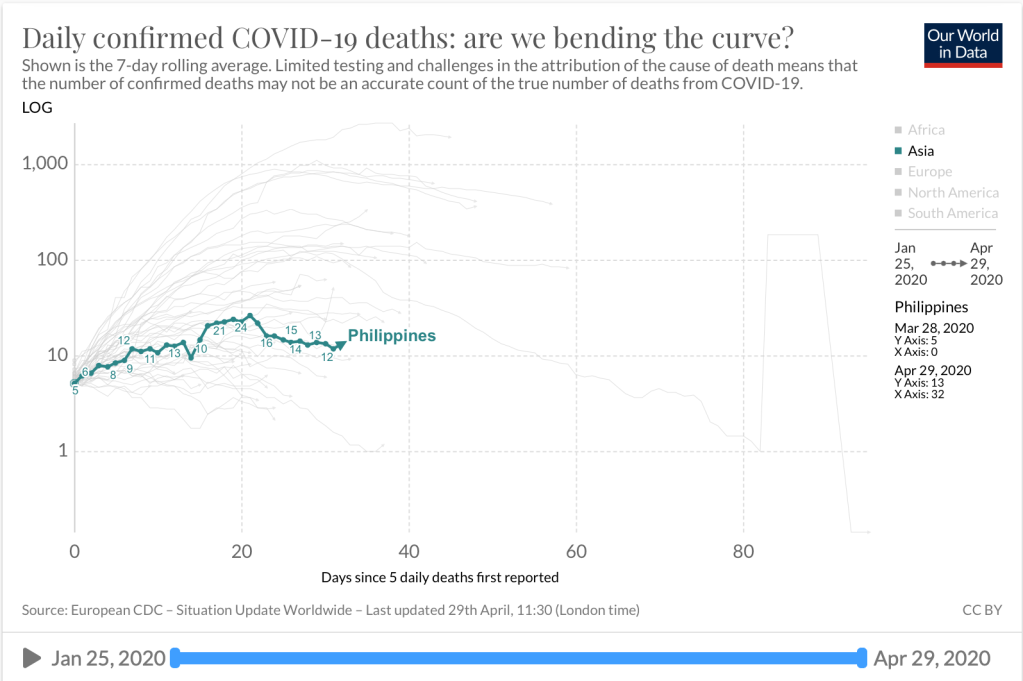
Figure 3 transforms the linear data into a logarithmic scale. It reported its 5th death on March 28. On the 20th day up to the publication of this article, it has remained above 10. Those numbers need to be “bent” in order to see the impact of the ECQ on death rates due to SARS-CoV-2.
So why do I feel that we’re into the perfect storm?
As a general rule, COVID is not the only health problem we currently have. The nonCOVID cases, far outnumber the Coronavirus cases. In short, SARS-COV-2 or COVID-19 has served as a major distractor in seeing the real health picture of the country. At the beginning of this storm, we were battling poliovirus. Last year we hardly recovered from the onslaught of measles and dengue. One infectious disease after another. Where are we now with cases of polio and dengue and measles? I would appreciate it if someone could give us clear data that the war against COVID is a far greater one than other vaccine preventable diseases. After all, at the current crisis, I am sure that the Department of Health has all hands on deck with COVID. We also need clear data on the other noncommunicable diseases (NCDs) and the mortality from NCDs.
Based on published data from the Department of Health’s website, http://www.doh.gov.ph/mortality in 2013, there were 531,280 registered deaths from all causes in all age groups. That’s an average of more than 44,000 deaths a month. Deaths mostly came from the most dense populations – 13.4% from NCR (71,050) and 14.3% from Calabarzon (75,743). How are the 558 deaths (from January to April 29, 2020) from COVID-19 impacting the overall health care of the Filipino people? Focusing our attention solely at COVID-19 is poor planning in the allocation of health resources and healthcare because the greater majority (those with cancer, heart disease, on dialysis, had a stroke, accidents, infants with sepsis, dengue, etc.) will need equally, if not greater attention, than COVID cases alone.
June is fast approaching.
And the onslaught of the rainy season brings with it a cycle of other infectious diseases the present in a similar way as Coronavirus would present at the onset of illness.
Fever. Colds. Chills. Cough.
Dengue. Measles. Seasonal Flu…to name a few.
Hence the urgency in getting out of this pandemic really quick.
It is a difficult and arduous task ahead for the head of state to bring its people out of this pandemic. But it needs to be done in unison. It needs to make policies based on worthwhile real-time factual data that is not confusing. People in government cannot just make senseless statements that there’s nothing we can do about this pandemic because there is. Other countries are able to bring down their mortality rates and eventually the cases by doing more testing and channeling more resources at contact tracing and practical measures in isolating those who come in contact with positive cases.
While it may be a tall order, it is one that requires a sense of urgency not only through ECQs or praying that a cure or vaccine be made available soonest. The most practical and doable is getting the numbers right from the get go. Only then can we make valuable and sensible plans on how to win the war against this virus.
I cannot overemphasize the urgency in getting out of this Coronavirus pandemic. Otherwise, like a ship that sails into a deep vast unknown ocean with no tracking device, we’re heading into the perfect storm.