They announce the summary in the evening…but the specific data in the Data Drop are not available until 10AM the following day. So here”s what happened yesterday and announced at 8PM last night.

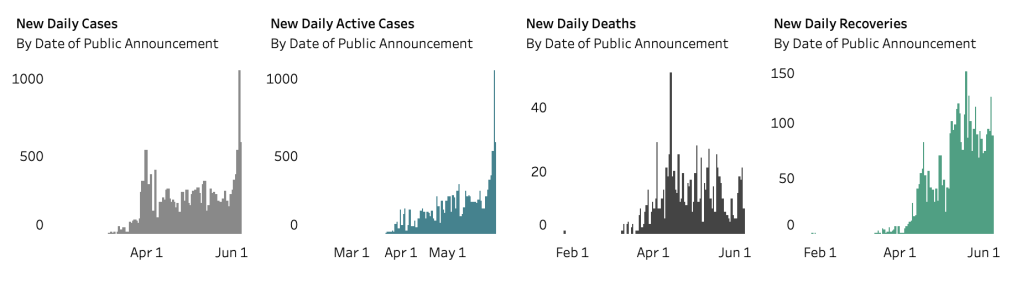
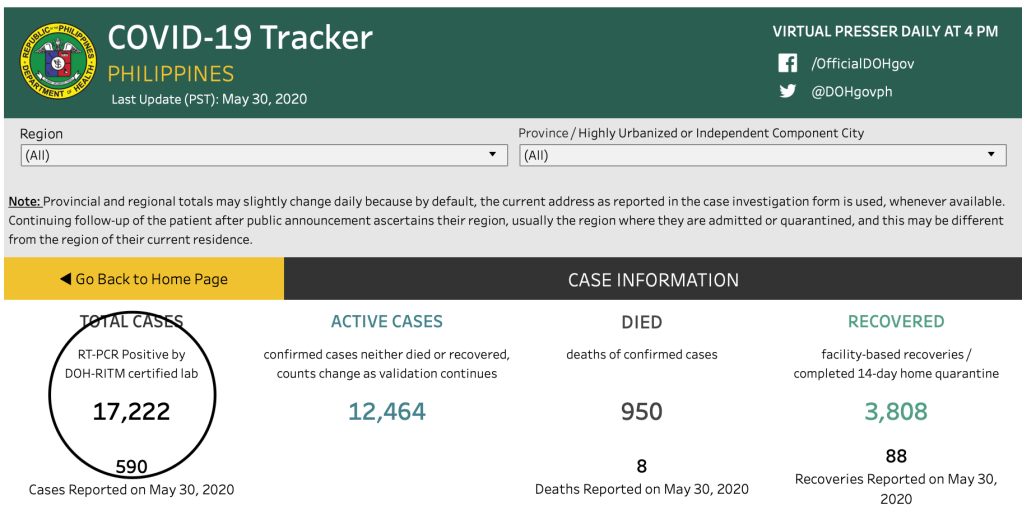
Their “fresh cases” today are up at 252 from 46 the previous night. The “late cases” (> 4 days into validation) is 338 for a grand total of 590 cases reported last night – lower than the yesterday’s 1046 but higher than the previous day’s 539. There were 8 deaths and 88 recoveries reported, bringing the case fatality rate to an all time low of 5.5%. Unfortunately, because of the higher number of confirmed cases (fresh or otherwise), the recovery rates have also been dragged down a low of 22.1%.
This change in the reporting system in order to address the backlog in data has sparked confusion, not only to the ordinary layman but to the medical community as well who’ve been constantly following the numbers in order to craft policies at the workplace (hospital or business) as the GCQ (general community quarantine) takes into effect tomorrow.
Unfortunately, it is what it is and we need to contend with what is in the Data Drop system.
Let’s the dissect the available data.
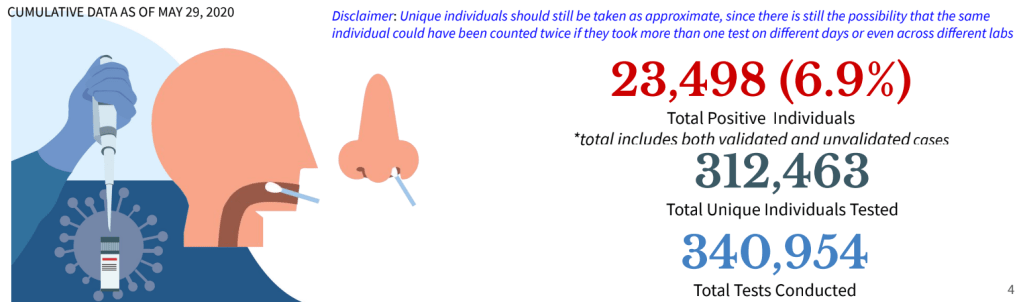
As of May 29, more than 340,000 tests have been conducted (+8138 tests done) in 312,463 (+7347) total unique individuals. Of the total number of individuals tested only 6.9% are positive. Or a total of 23,498 positive individuals (both validated and unvalidated cases). Since there are only 17,224 confirmed cases as of last night, there are around 6000+ missing positive patients. These may not necessarily be NEW confirmed patients but previously positive patients who have had repeat testing done, remained positive and are still up for repeat testing. It is also difficult to separate patients who have tests done in one facility and have repeat tests done in another facility. But since I am not privy on how information is collected for these patients, I am speculating that this may be a problem that the health agency is plagued with. Validating this kind of information is labor intensive and leaves no room for human error. Elaborating on this discrepancy by the agency should allay the public’s fear of why the numbers have recently gone up.
Consistency and accuracy in data is vital to any report or pronouncement by the agency.
When they announce a total of 17,224 cases in their summary press release last night and yet in their own website announce this, you know that we have a problem even in validating the official information that is dished out by the agency.
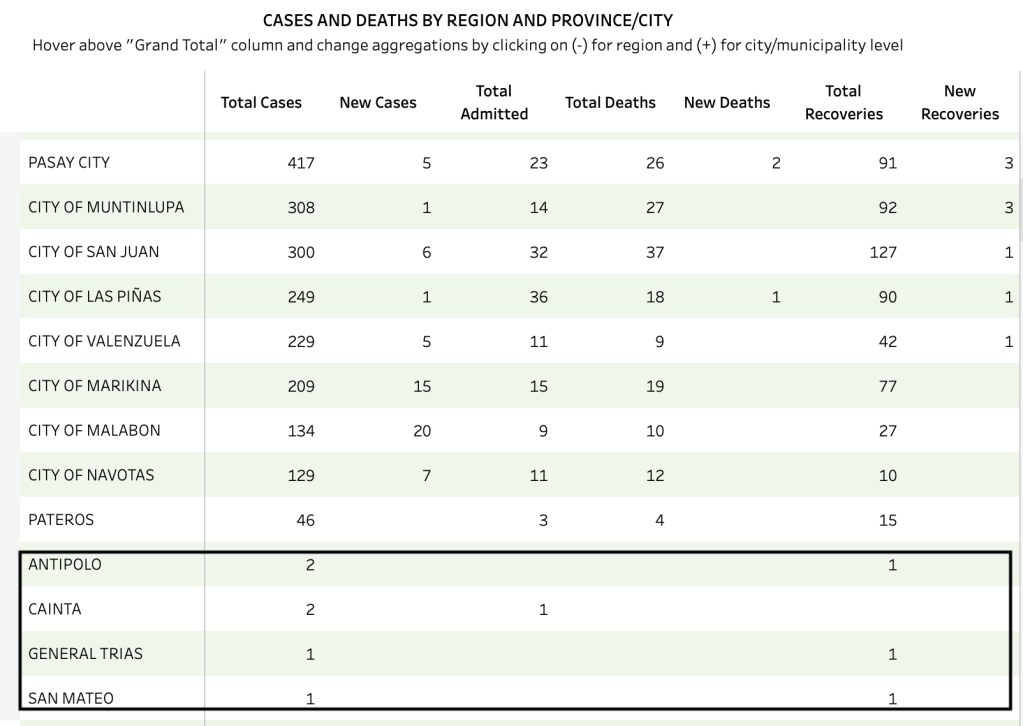
Of the 252 “fresh cases” and 338 “late cases”, 162 and 218, respectively came from the National Capital Region. This makes a total of 380 cases from the NCR alone (fresh or otherwise). There is no breakdown on which are fresh or late but of the 380, 236 (62%) are still for validation. Those validated are: Caloocan City (27), Manila (20), Malabon (20), Marikina (15), Quezon City (12), Navotas (7), San Juan (6); Valenzuela, Pasay City, Pasig, and Makati with 5 each; Taguig (3); Parañaque (2), and 1 apiece for Las Piñas and Muntinlupa.
What I don’t get is how these places got included in the NCR as separate cities.
Region VII reported 18 fresh cases. There were no late cases reported. The only conclusion one can make from this is that (a) there’s no backlog in the Region VII data and (b) all the data yesterday – 11 from Cebu City and 7 from Mandaue are within the three days window.
The 9 reported repatriates are all late data (> 4 days ago).
The remaining 183 (72 fresh and 111 late) are a basket of information where you cannot discern which are “fresh” and which are considered “late”.
Region IV-A for example has 29 data for validation while those with reports are from Rizal (4), Laguna (1), Cavite (4).
Region III (Central Luzon) has 4 for validation with confirmed reports from Bulacan (5), Bataan (1).
Region VI reported 1 apiece from Iloilo Province, Antique and Bacolod City.
Region I had 1 case from Pangasinan and 2 from La Union.
The Bicol Region (Region V) has 4 cases for validation but reported 1 from Albay and 1 from Camarines Sur.
Region IX reported 1 case from Zamboanga City.
Region II (Cagayan Valley) reported 1 from Isabela.
Region IV-B (MIMAROPA) have 2 cases for validation still.
Region XII has 1 reported case from General Santos City.
And there are 117 cases for validation from – well, your guess is as good as mine.

I am surmising (again) that these for validation (for validation) are probably patients without tagged residences. Again, as to why there is no information on them needs to addressed by the health agency. Perhaps informing the local government RESU on the completeness of the documents submitted to them should be the rule rather than the exception. Actually, for awhile there, the Department of Health was able to consistently provide almost 100% tagged residences especially during late April to mid-May.
Finally there is the BEAT COVID informatics they provide. While there is a wealth of information there, the barrage in information that may not be totally relevant to the public is difficult to keep up with.
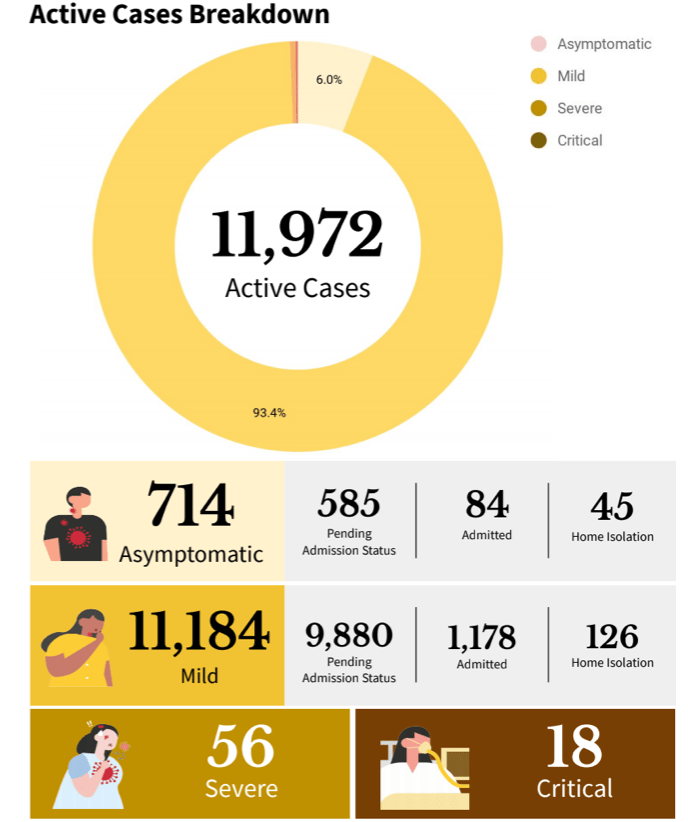
For example, under case breakdown of ACTIVE CASES as of May 29, it is good to know that most the active cases are actually mild (93.4%) and that the asymptomatic comprise only 6% of the total cases. As of this date, 56 have severe illness and 18 are critical.
In the same Philippine Situationer https://drive.google.com/file/d/1cDD9G8QKK_y5Bc3o6Pq5k4fXGYhkCVkx/view, I get confused at the available beds and mechanical ventilators dedicated to COVID-19 cases.

If there are only 18 critical (let’s even throw in the 56 severe) cases among the active cases, why are 358 mechanical ventilators in use and 463 ICU beds occupied? This is under the heading of Hospital Beds and Mechanical Ventilators Dedicated to COVID-19 CASES!
While I can feel how overwhelmed the health agency is, pointing out these inconsistencies is intended to make them aware that people are following them. After all, who else can we trust our health if not from our health agency?
Integrity of data is vital to every healthcare system. After all, it is the basis of policies made by the government.