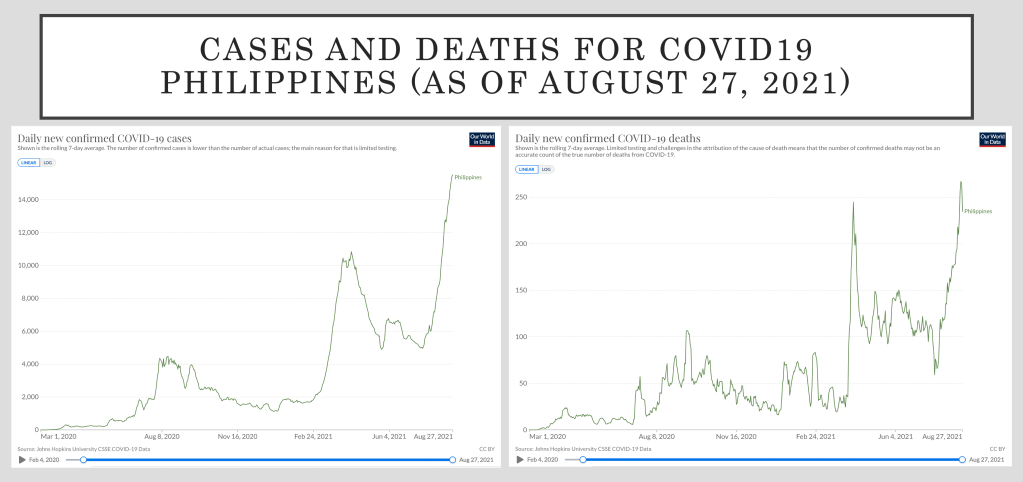
While we had lesser cases today than the two previous days, it was still the third highest number of new cases announced since the pandemic began. The active cases are now past 125,000.
With 16,044 new cases today, the Philippines officially passes Iraq and sits in the 21st rank among countries with COVID-19 cases.
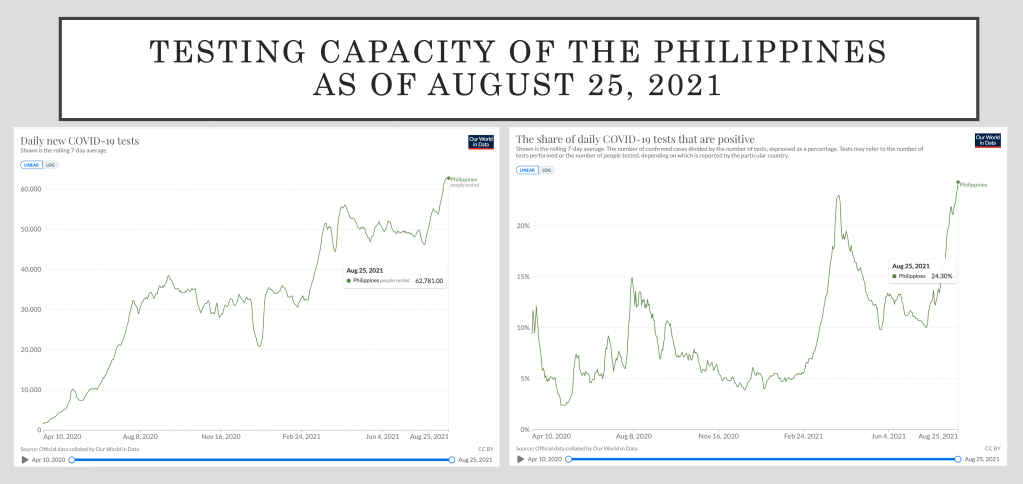
There were more than 65,000 tests done last August 20, but in spite of the slightly higher testing done, the positive cases are still past 25%. One in four tested that day tested positive.
The Health Agency adds 215 new deaths today, putting the case fatality ratio for outcomes at 1.86%. It is important to remember that of the 1,839,635 officially reported COVID-19 cases, only 1,713,735 patients had outcomes. Among the latter, 98.14% have fully recovered. The active cases should be left as active cases with no outcomes. Yet.
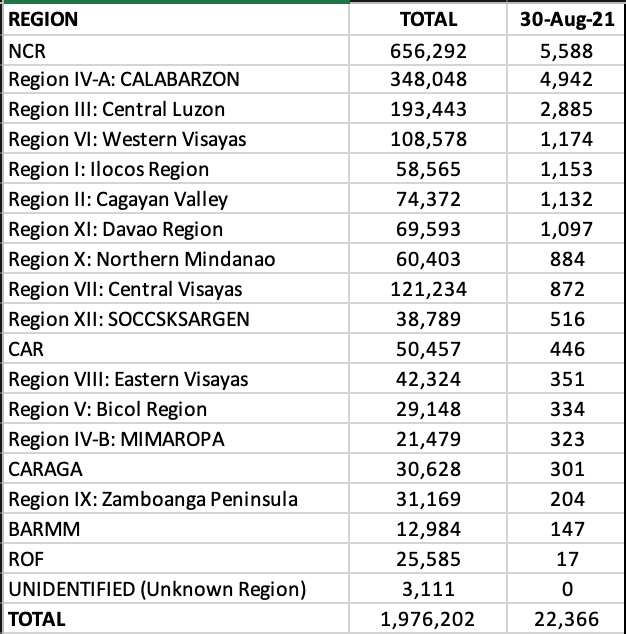
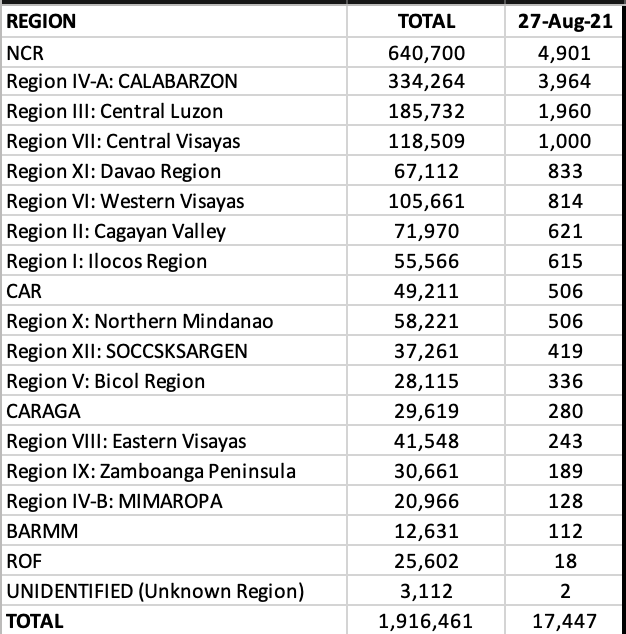
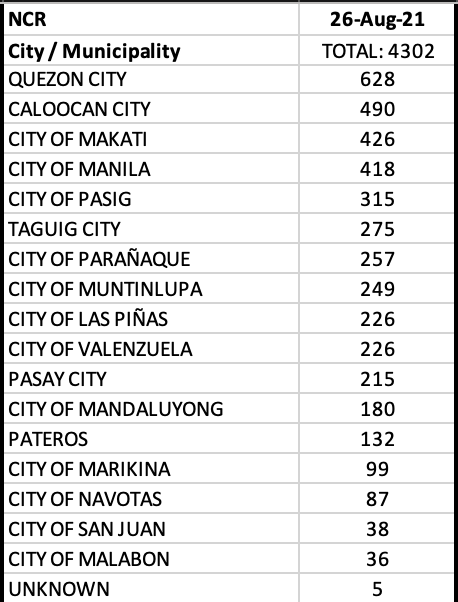
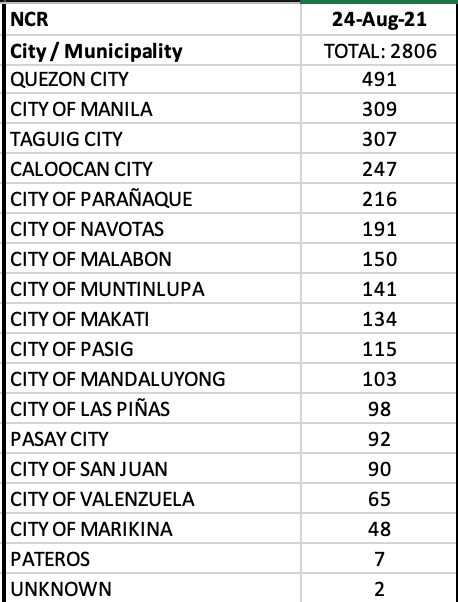
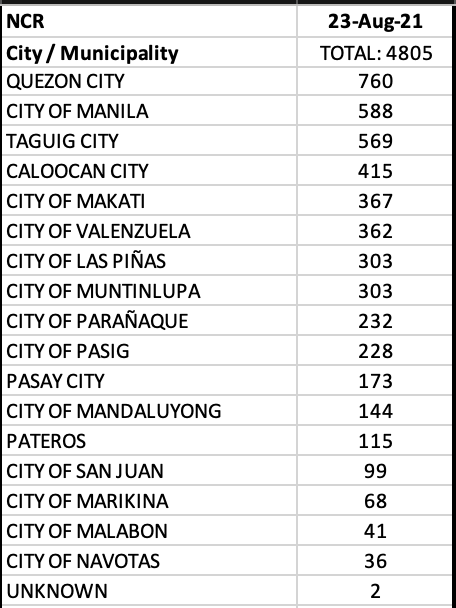
NCR recorded a decent 3,973 or 24.7% of the total cases in the country. CALABARZON + Central Luzon + Central Visayas accounted for an additional 44.5% of the cases.
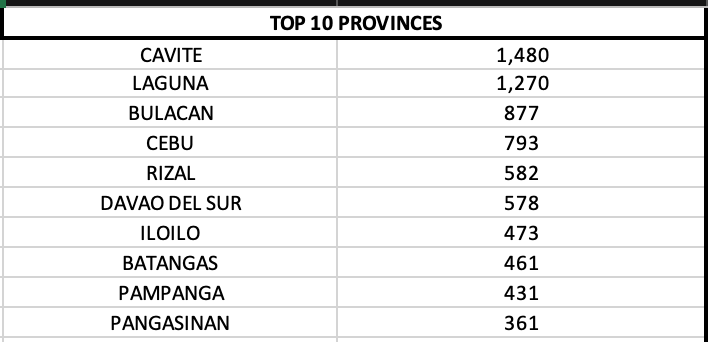
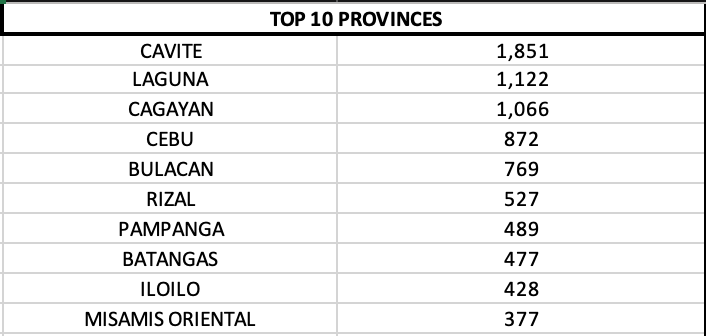
On a provincial level, Cavite, Laguna and Cebu reported quadruple digits.
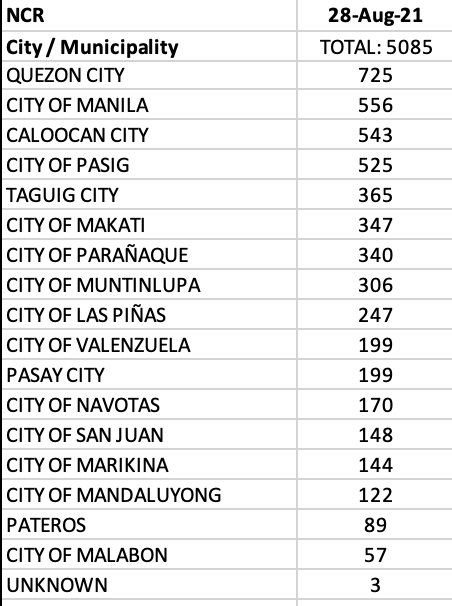
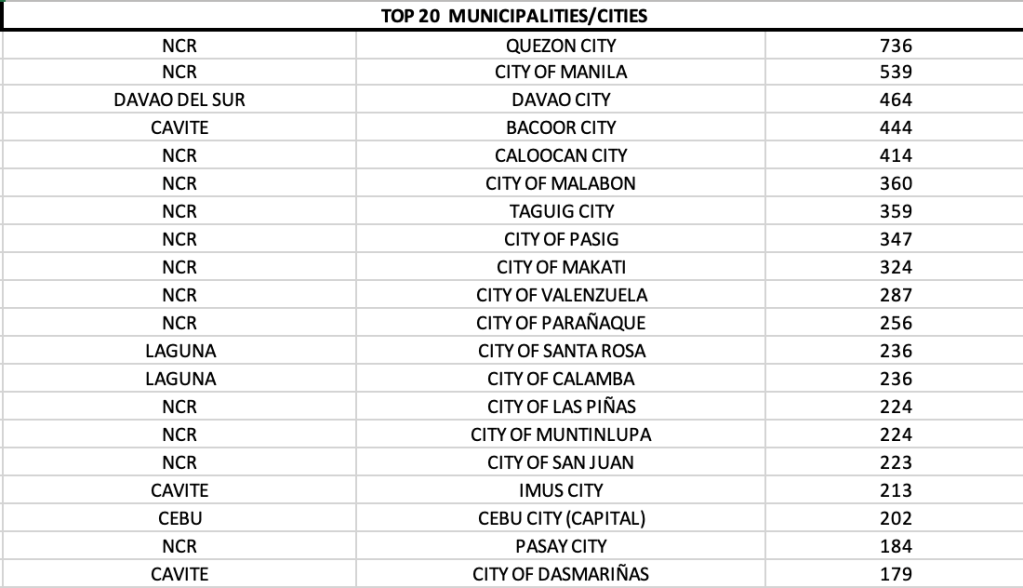
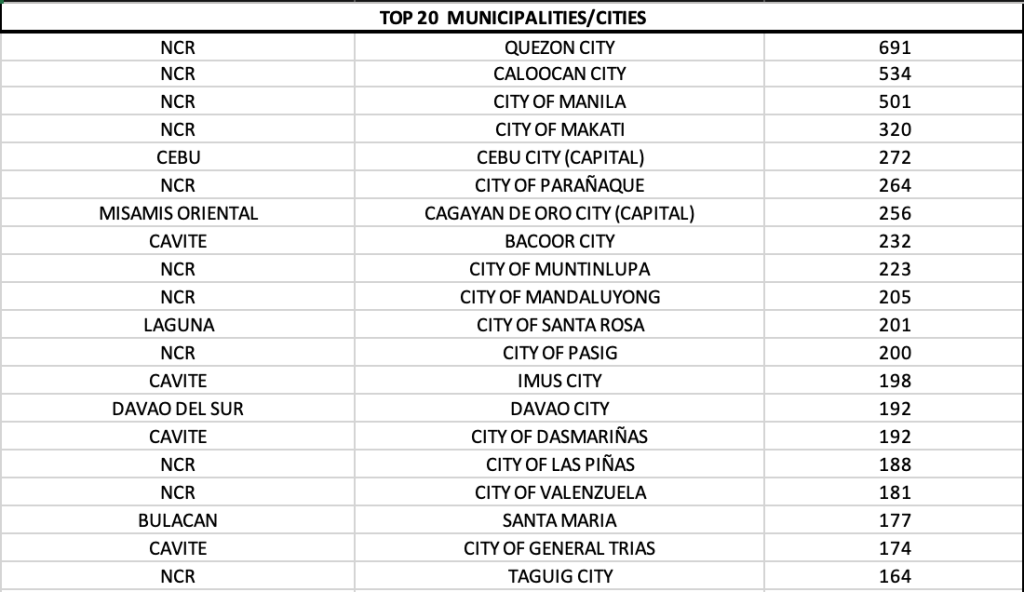
Eleven of 17 LGUs in NCR were in the top 20 cities with most cases, led by Quezon City. Four LGUs in Cavite were in the top twenty as well.
OCTA MONITORING REPORT
As the government began to lift a tighter lockdown in our rollercoaster ride of lockdowns, the growth rate in new cases declined a tad. While the growth rate continues to increase, it has slowed down. Which is like saying, yes the cases are still rising but not as much as the week before. The NCR now averages 3,819 cases daily (August 15-21 week) compared to the 3,088 daily cases for the week before (August 8-14).
The Rt is down at 1.67 in NCR (versus 1.9 last week), but it is still high. Very high, as a matter of fact.
The average positive rate in the NCR is at 22% at critical levels. That’s because mostly the symptomatic get tested.
The data shows you one thing. Two-week lockdowns don’t work.
Here’s a typical household scenario.
There are 7 people in the home. Two senior citizens, the parents, two children and a maid. The grandfather comes down with COVID-19. The family gets swabbed. They are all negative. They isolate the grandfather. After five days, the grandmother has fever. She gets swabbed again. She is now positive. The remaining 5 in the household get swabbed again. They are negative. After five days, the parents are now coughing and have low grade fever. They both turn up positive after getting swabbed. The kids and the maid who were swabbed remain negative. But they continue to be exposed to the parents because the children are 1 and 3 years old, respectively. After 3 days, the kids now have a runny nose and some diarrhea. The maid also falls ill. They all get swabbed. Again. This time they are all positive. More than two weeks has passed before the whole household is not fully infected.
Depending on the size of the household, transmission will continue to occur between 2-4 weeks. It is best to always presume that it takes 4 weeks for a typical household to recover. Extrapolating that to a community, depending on the size of the community, it would normally take 1-2 months for the whole community to stop circulation of SARS-CoV-2. Locking down a street or a Barangay for two weeks will most likely fail.
The two weeks ECQ did not really bring down the cases. It slowed it down, based on the numbers of the Health Agency. As to the accuracy of the data, that is another challenge during the pandemic of perpetual lockdowns.
There is a need to place more science into the anatomy of a lockdown. While it is challenging to the business community, it is, sad to say, a bullet we need to bite. Resources from the national and local governments must be used properly to assist people survive for health, personal needs and livelihood during quarantine. The goal of a lockdown is not to simply slow down the viral transmission in the community. It is to starve it dry. And it is understandable that economics plays a large role in every lockdown.
While vaccines may help in decreasing the severity of infection for patients that eventually get infected, it is not the only solution. It is apparent that the mix messages sent out by the health officials and those that create policies and implement them get lost in translation.
Every surge should prepare us for another surge. As they say, all pandemics come to an end. It is how we handle a surge that matters most. We need to steer back to the science of the virus, incorporate the economic repercussions, and enhance the pillars of controlling the pandemic by testing, tracing, isolating/quarantine and vaccination.
THE WEEK IN REVIEW
While OCTA showed an over-all slowing down in the rise of cases in the NCR, the number of new cases continue to increase daily. The slope is a very steep one for both new cases and newly reported deaths.
As a matter of fact, if one looks at the report of the Health Agency on case fatality rate, the DoH downplays the rate by using the total cases in the country as the denominator. That is why we have a 1.73% case fatality rate, according to the infographics. But with more active cases, we really do not know what their outcomes will be. And it would be premature to presume that all will survive, when in reality, many factors can play a role in poorer outcomes especially if the healthcare utilization is overwhelmed.
The moving-average CFR in reality stands at 2.14%. A 0.41% discrepancy from what is reported daily.
While testing has slightly gone up, we still lag in testing patients. Lack of testing results in poor contact tracing. For now, most of those that are being tested are the symptomatic cases. Rapid antigen testing, which can, and should be used during the outbreak are still not being used by the agency. If it is, it is not being recorded because all the announcements are based on RT-PCR test. And while the claim that there is better sensitivity with the RT-PCR, like the rapid antigen tests, a negative test today will not guarantee you a negative test tomorrow. If the government is really bent on conversing the scarce resources, it should begin to utilize rapid tests as a screening method together with RT-PCR in instances when the latter needs to be used.
The reproduction number among select Asian nations as well as their 7-day average cases are provided in this report. Notice how Indonesia has worked well at slowing down its cases by keeping its reproduction number below 1.0.
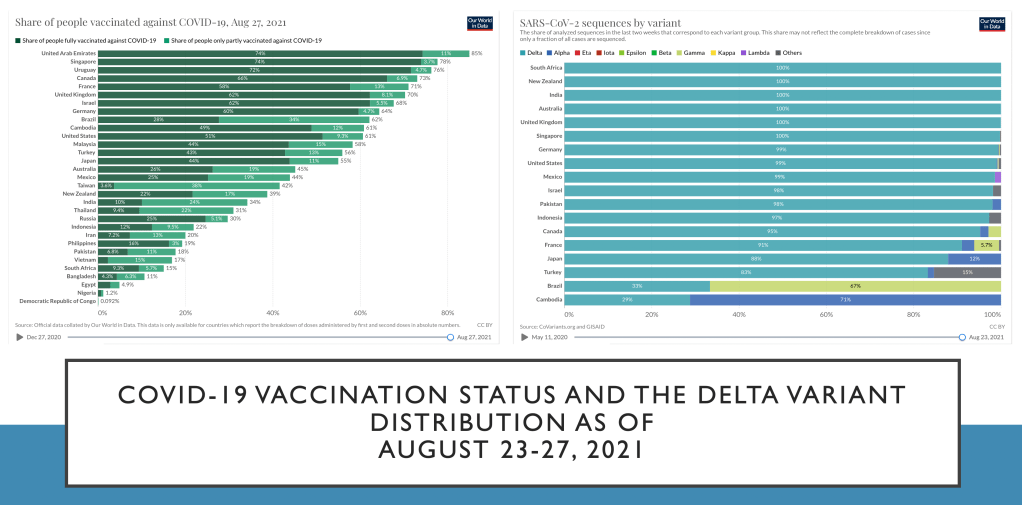
The state of vaccination in many parts of the world is provided in the final infographic. The delta variant has proven to be a formidable challenge, as many countries report this variant as the predominant circulating type for SARS-CoV-2. Undoubtedly, in the Philippines, delta has landed as well and is now in various communities.
Less than 1/3 of the world’s eligible population has received a single dose covid vaccine as of this report. It’s even lower (less than 1/4) when you take into consideration those that are now fully vaccinated.
The scarcity of vaccines, the gap between wealthier vs. poorer nations in access to the vaccines, the issue on waning immunity to previous vaccines, and finally the efficacy of some vaccine platforms versus delta variant has played a major role in the current surge.