There is a saying that goes “it’s hard to teach an old dog new tricks“.
And there’s no better situation to apply that saying than today – the COVID-19 pandemic in our midst.
When the various phases of the enhanced community quarantine begins to ease up, the question is – when do we go back to our “usual” normal lives?
By nature, every animal is a social being. Even the lowest form of animal engages in some kind of social interaction. From time of conception, our interaction with another life form is deeply ingrained with the attachment of that umbilical cord. Growth and neurodevelopment milestones are dependent on human interaction with both the environment and other beings in our midst. Humanity evolves because of social interaction and adaptive behavior.
It’s difficult for anyone to even imagine living in a world where the new norm means having to don a face mask each time you step out of your home, stay a meter away from another person, and avoid crowds and other social gatherings.
The last decade saw the boom of social media. Where friends were virtually in touch with one another through Facebook. Or where one’s opinion was simply Tweeted into the air. Or where food and travel places were Instagrammable. Where likes and shares were the norm rather than the exception.
As we were just getting settled into planning our annual vacations, post our successes and failures, and organize our future – a lowly respiratory virus perturbs our social milieu.
So how do we gradually settle into the “new normal”?
Over the past days, an article came out suggesting that experts ranked 36 activities risk level during the pandemic https://www.al.com/news/2020/06/from-hair-salons-to-gyms-experts-rank-36-activities-by-coronavirus-risk-level.html. It’s an interesting read, but let me put my 2 cents worth on that article by making it simpler for everyone to remember how to calculate those risks and eventually incorporate into our daily lives.
I guess the ‘no brainer’ here is we start by changing our daily routine. There are things we do that put us at highest risk in catching the virus. Knowing the extent of risk can help workplaces, schools and homes adjust activities of daily living to help us lower our risk to getting exposed to it. After all, it will be quite awhile before we get to see a vaccine or treatment (if there ever will be one).
On an individual capacity, we should decide for ourselves which places we should avoid and which ones pose little risk of getting infected from the virus.
There are basically five factors when it comes to risk assessment: (1) indoor or outdoor activity, (2) exposure time, (3) how likely we are to comply with the risk presented, (4) social distancing, and (5) personal risk level.
As a general rule, activities outdoors are generally safer because the virus does not get recirculated especially when the space you converge in is large.
Activities that don’t allow social distancing are riskier. Because the infection is acquired from droplet transmission. Activities that involve singing and shouting should be avoided for the meantime.
Exposure time is an important factor as well. Casually walking by a person along the street who may be infected with the virus is less risky than being seated beside someone in the mall or coffee shop the next 2 hours waiting for your friend to arrive.
Then there’s the risk on a personal level. If you know you belong to the vulnerable group (have comorbids or health risks that make you susceptible to getting infected), you should know better than anyone else on what steps to take.
Assign a score between 0-2 for each of the factors provided. 0 meaning no risk, 1 for intermediate risk and 2 for highest risk. Add up the factors with the scores and anything that puts you between 0-3 should be lowest risk, 4-7 as intermediate risk and 8-10 for highest risk.
Bars and Brothels
Now that’s a definite 10. And it’s worse if there’s even smoking, vaping and a lot of socializing. Who’s even going to bother wearing a mask inside a bar?
Adding the strippers and those gyrating men and women in scanty clothing (wearing a mask?) isn’t really the kind of stuff people trek to watch.
When the crowd gets rowdy, and they definitely will with all that booze and most likely drugs, that’s enough to become loose to keep your guard down.
It’s not only COVID-19 that you’re going to catch in a brothel, it’s more likely that you’re bound to even get pathogens that are sexually transmissible. Either ways – you’re going to die faster.
Concerts
Not too sure with anyone who’s willing to pay P100,000 to see someone sing and dance because the 10,000 seater venue can only allow 1,000 people -seated 2 seats apart on the side and two seats apart front and back.
But that would defeat the purpose of having the performer even get a standing ovation from a jam-packed audience all wearing a face mask. Or have a jam-packed audience rub arms, elbows, crotches and butts against each other singing, screaming and gyrating to the music and the show.
Definitely a risk level of 10.
Sports (and Gyms)
Definitely a no-no when you’re going to be splattering saliva and sweat against each other. So gyms for that matter should remain closed for the time being unless you can make sure that you allow only 3-5 people at a time (which is impossible to do) and that people are limited to working out by appointment and at a designated time limit (1 hour maximum) instead of parking their whole day inside the gym.
Reopening the gym will be a nightmare considering that you will have less manpower (gym instructors) and will need to make sure that all the equipments are cleaned after very gym rat uses it. But that’s hard to do because some of them jump from one equipment to another and then back to the same equipment for a routine for the chest, the back, the legs, the arms, the trapezius muscles….and cleaning up with sodium hypochlorite after every person using that piece of metal is potentially toxic.
And those spin, Yoga and Zumba classes will need to go for awhile. If you need to burn those calories, walking/running outside is healthier than doing it on the indoor treadmill (which is probably located less than a meter from the next treadmill in a 200 sqm size gym).
Anything that will require huffing and puffing for the whole duration of the activity will need to stay closed for awhile, unless you can make sure that the place is immaculately clean.
But let me put that in another context. If you won’t allow your kids to go to a park to mingle with other children who run around in the wild, or take your children to Fun Ranch because you’re afraid of who had the last touch on that slide, then the gym is the equivalent for the big boys (and girls) . For gyms, I’d give it anywhere between 8-10. Depending on several factors how they’d probably assure that there’s never going to be a crowd or that every piece of equipment is going to be cleaned down after every use or that there will be limited use and access by every customer or that the locker rooms won’t even have fomites and will be kept to a distance between one user and the next.
Any contact sports is definitely out of the reopening bid. Basketball, wrestling, volleyball, football, soccer, rugby, martial arts, boxing…they should be in park-mode for the meantime as they are a definite 10!
Sports activities in open spaces where people are far apart from one another (golf and outdoor or open-space tennis) carry very low risk. As long as socializing is not within the agenda, then it should pose a risk between 0-3.
Swimming is controversial. That would depend on how close you probably are to the next person. As a general rule, if you have a pool at home, swim there. If you want to use a public pool, then that would entail risks depending on how large the pool is and how many people are in the pool that given day. Even if the pool is chlorinated, you cannot help when people splatter saliva and blow air bubbles after several laps. Because we don’t know how SARS-CoV-2 is transmitted when swimming, it’s best that if and when we need to swim, consider swimming in a more open space like the sea or ocean. Of course, the ideal would be if you had a private beach…and that would put the risk to totally ZERO. In the meantime, the ordinary folks like us would have to contend with risk between 4-7 when swimming in public places.
Parks and amusement centers
They’re meant to draw a crowd. Especially those themed parks. The photo-ops. Those instagrammable moments. Yup! They’re definitely a perfect 10! It’s just not a fun place to have no parades anymore in the amusement park.
Then there are the private parks in the enclaves of the upper class of society. As long as the nannies there don’t congregate to exchange juicy stories with their wards in tow, these pose lower risks than the themed amusement centers (Enchanted Kingdom, Disneyland, Universal Studios, etc). I’d give the public amusement centers anywhere between 8-10 while the private parks in the various villages a 3-5.
Schools
Definitely high risk.
And I base that from experience in dealing with kids. Children are social animals. Adulthood is different from childhood.
Parents worry about not having to send their kids to school because it would mean one year (or longer?) loss…and I get that. However, schools are complicated when it comes to the risk for spread.
Each year, when the flu season comes, it’s also when our clinics are full to the brim. With kids coughing, sneezing, colds, sore throat and fever. The flu shots help diminish the risk of getting flu but it’s not 100% protective. And there are other respiratory viruses you need to contend with. The best way really for children not to get sick is not to go to school, because let’s face it – school is after all one of the biggest Petri dish in the world. But that’s a no-no. And somehow, they’ve got to get their education back on track.
The problem is, how do you get the smaller children (and yes even those teenagers that need to “hang out”) stay separated, wear a mask or even wash their hands well. Seriously, hygiene is the last thing that they’ll even remember.
Let’s put a little scientific evidence to this. As of June 10, 2020, of 22,992 data points (individuals positive for SARS-CoV-2) in the Philippines, 573 (2.5%) kids 0-9 years old, 1012 (4.4%) children 10-19 years old, and 4492 (19.5%) school-aged adults 20-29 years old comprised part of the total patients who were positive for the virus. That means that 7% belonging to the 0-18 years old age group alone were positive for the virus. If we threw in the college students and the age group that would potentially attend postgraduate studies, 27% of those less than 29 years old were positive for the virus.
Restarting school should not only benefit those who send their children to private schools. The public school system is the larger community we need to draft guidelines for. After all, the private schools will be able to manage this better than those kids who go to public school. But the public school system is more overwhelmed with more students per class than private schools. And more challenged because majority of its students have the least access to a stable internet connection, let alone a tablet or computer.
School opening should be an all-or-none phenomenon. We either start school or we don’t. Because it will not be fair for those who have less in life compared to those who have more.
A hybrid model can be studied. Face-to-face may not be required daily and classes can go in shifts for face-to-face engagements. Students can be divided into 2-3 groups (or even 4) and be seen every day of the week per month with the rest being seen online or having tasks and assignments conducted online. However, this may be challenging to apply to those that are 8 years old and below. Getting all the school children without having break periods is ideal so that immediately after classes, they are sent home.
Because of the challenging task ahead – this gets an 8-10 on my meter scale.
Church
In a country where more than 80% of its total population are Catholics and where celebrating Holy occasions is the rule rather than the exception, the devotees definitely miss the physical presence and ambience of our churches.
But one can’t help point out the fact that the two outbreaks in Singapore and South Korea came from churches. The one in the Philippines started from a mosque in San Juan City.
It’s totally different when the mass is online compared to having the priest celebrate mass in front of us and receiving holy communion.
The only issues with mass are the social distancing and the singing. Yep, singing. While it is best that songs of joy and peace and happiness and veneration are offered to God, singing is also one of the most aggressive way of transmitting the virus. That, and a lot of people verbalizing together. But masses can be held without having a person sing (it can be a minus one or a taped song for that particular segment of the mass), and that people don’t need to respond verbally to every sentence of the presiding priest. For now, we can be a passive audience and quietly shout out (in our mind and heart) the responses. After all, when we come from mass, it is the deep faith and practice of that faith that counts the most.
The churches can continue to offer online masses for the faithful that may be vulnerable and challenged to physically attend mass. Because of the limited number of people that can physically come, if possible try to offer more masses a day.
Risk level for churches? 4-6 depending on the capacity of the place of worship.
Movies
The advent of Netflix, Viu, iFlix and other downloadable sites has changed the entertainment industry dramatically. We now get to enjoy the “movies” within the confines of our homes – when we want to. Some homes even have their own room dedicated to an 80″ screen and surround sound! Seriously, I don’t think a lot of us would have our sanity intact during this lockdown were it not for these entertainment sites.
Movie houses, like concert halls will need to practice a lot of social distancing (as people will need to sit down for hours) and all will be operating at a loss unless they charge exorbitantly just to watch a film. It’s also going to be challenging sharing that bucket of popcorn a meter away from one another or even being intimate between seats.
In this day and age of digital technology, going to the movies is in the least business priority. With a pandemic that isn’t going to go away anytime soon, the return of the indoor movie houses will probably take awhile.
The risk level? 6-8 depending on how well prepared they are at keeping the place immaculate show after show.
Hair salons
It’s impossible to keep a social distance with barbers and hair stylists. But it’s the same line of reasoning I would dare say – that it’s impossible to keep a social distance between the dentist, the doctor, the veterinarian, the bank teller, the supermarket cashier, the gasoline boy, the market vendor…
Because any face-to-face interaction is RIGHT IN YOUR FACE, and you just need to make sure that we wear a mask (or include a face shield if you must) and keep the chit chat to zero. Go get your hair dyed and make the hair stylist leave the premises after coloring, return to have it washed, then voila, you’re done.
The article on AL.com suggested that hair dryers shouldn’t be used because it could potentially circulate the virus. I am not too sure where that idea came from and what ballpark they actually live in, but seriously, if everyone is wearing a mask, what virus to circulate are they even talking about?
A haircut will not usually take more than 15-20 minutes. But it’s the same amount of time (or even shorter) than a face-to-face appointment with a healthcare provider.
Similar to health care clinics, salons and barbershops should be BY APPOINTMENT ONLY. The waiting areas can be closed off. There should also be no simultaneous procedures that will require the whole salon staff to be at your hands (manicure), feet (pedicure), head (shampoo and haircut), and face (make-up artist). Now that, is a crowd.
Remember, part of hygiene is good grooming. So yes, open those barbershops and salons but make sure to keep the risk low by taking these pointers into consideration.
My risk assessment is salons and barbershops would be between 3-4.
Dining and restaurants
If there’s one business that has been extensively hurt during this pandemic it’s the food business.
From the make shift food stand to the fine dining places, these were businesses that became a challenge to survive the lockdowns.
Luckily, they could still operate using “take outs” or “deliveries” as part of the “new normal” in their business setting. In my observation, the food deliveries and take outs had lesser portions or ended up more expensive. They were charging for the containers as add on to the orders. Which I found unfair. In the first place, these foodies were not operating with dishwashing machines and busboys any longer. There were lesser staff and lesser utensils to clean. In short, their operational costs are much lower. To pass on additional cost to customers in order to meet the same profit margins as BEFORE a lockdown is called greed.
The other day, I ordered take out from a Japanese restaurant and they charged 10% additional to the total bill for two dishes! So that means that if you order food worth 1000p, they’d still add 100p on top of that. Seriously? Talk about taking advantage of the customer! I mean, yes you need to survive. The question is, don’t we all?
So yeah, we go back to the point, how will these restaurants survive?
Similar to other establishments, dine in should be allowed but on a BY RESERVATION ONLY basis. If the space can accommodate 100 people, then the accommodations should be cut by 50%. Tables and chairs spread apart. All food should be ala carte and NO SHARING of dishes. Buffets are definite no-nos.
The requirement by the IATF of installing acrylic or clear barriers between customers is a bit too much and off. First of all, it makes no sense in having a barrier between people in one table. I understand that no one eats with a mask on and therefore placing barriers will minimize the splattering of saliva and transmission from droplets during a conversation, but the barriers in itself will be a potential source for the virus to adhere to after every customer leaves the dining table. So it will need to get cleaned, wiped and dried before the next people come in. Tedious, taxing and well…unnecessary.
I still have to find a scientific paper that provides evidence that acrylic barriers help control the transmissibility of the virus. Since there is none, that’s another white elephant and an extra expense for the business.
I think more importantly than just making sure the dine-in restaurants practice good hygiene, is to make sure that people don’t park their bodies there. If I were to allow Starbucks and other coffee shops (and yes, even restaurants to operate already), all wi-fi access should be turned off and people should not be allowed to bring work and laptops for use in these places where they park their lives, sip a cup of coffee for the next two hours, or use it as a destination to have pocket meetings with clients.
The risk verdict? 3-5 if the above recommendations are all met.

Air Travel
We all want to get on that next flight to our fave destination.
The tourism industry has seen the worst outcomes during this lockdown and it’s really hurting the economy.
The truth of the matter is – air travel was responsible for the pandemic. Any way you place it, the bottom line is – were it not for air travel, we wouldn’t be in this health crisis at all.
In spite of the warning signs, we kept our borders opened. The red flag was there. Three cases among foreigners with one death traveling from Wuhan. Their entry point was Cebu. The rest is history. We let our guard down. Because the president was partial to our Chinese neighbor.
That’s a large difference when we look at how Vietnam dealt with the pandemic. China is their next-door neighbor. They totally shut down the border and began testing patients that were found to be sick, walled-off villages that had cases and did aggressive contact tracing from the get go. They stopped all flights in and out of the country. Today, they have no case for the last 3 weeks and had zero deaths.
But that is all water under the bridge.
Reopening the airline industry is going to be challenging. The trouble with travel is that people will always declare that they’re “fit to travel”. All you need is one sick person on that flight and all hell breaks loose.
Wiping down the seats, making sure that economy class is not full (difficult for budget airlines and good luck to getting flights that will charge you rock bottom prices as they used to). You can lay out the economy area with one person allowed per row and every other row unoccupied for a 2-2 configuration plane. The shorter the flights the better. The long hauls will probably be a bit more challenging.
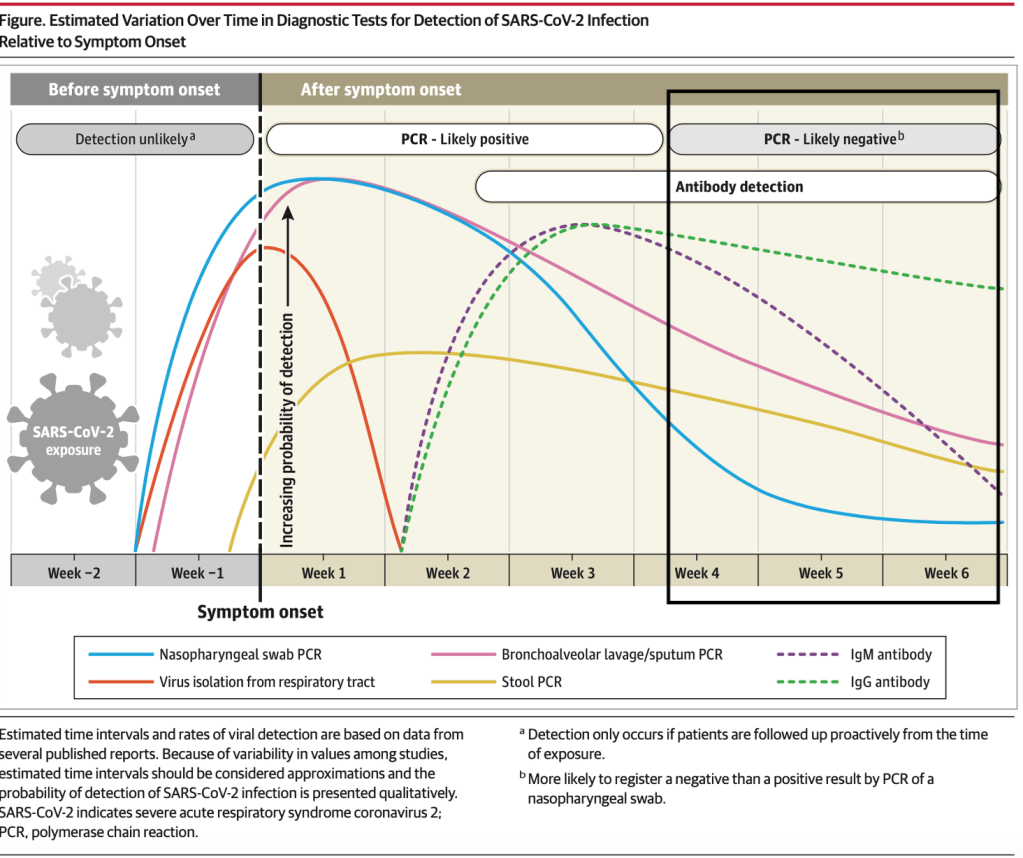
Will requiring swabs a few days prior to departure help? Not necessarily because if the patient is a pre-symptomatic, those swabs may turn out negative initially and by the time he boards the plane, he may have mild symptoms. And we all know that it’s difficult to cancel our flight bookings without getting penalties in the end.
The level risk? For short hauls, probably 3-5. For the long hauls, 6-8.
The malls
Like the supermarkets and the wet markets, it’s the crowd that matters. Going to the supermarket is an exercise in risk exposure. You can’t really help the fact that you’re one bunch of people congregating at the meat, fish and vegetable section. So yes, the supermarkets and wet markets are a definite risk and even though they wipe down the carts and take your temperature upon entry, it’s difficult to tell who had the last touch on the tens of thousands of goods you just picked up (and eventually returned and picked up again).
In the malls, as long as you’re able to separate people close to one another and maintain distance in the individual stores (like 2-4 people at a time depending on how big or small the store is), then the risk is going to be low. People will want to eventually fit the clothes they pick out. And people get icky over the fact that the clothes on the rack may be contaminated. But the likelihood that the virus will stay on the rack is very low.
It’s always best that if you know your size, don’t try on the clothes that you like in the store. Remember, during the three months quarantine period, you probably gained more weight that you think. So make room for that extra paunch. Pick a size bigger than what you used to wear.
When you get home, and you’re a tad paranoid, wash the clothes you bought.
And there should be a NO RETURN NO EXCHANGE policy, for everyone’s safety.
No mall sales and no other mall activities (like concerts or fashion shows or gigs or promos) should be in place.
My level risk if these are observed for the supermarkets? A definite 6-8 depending on the staff and size of the supermarket. For the malls and stores? Anywhere between 3-5.

The hospitals and medical clinics
It is obvious that the biggest misconception among the lay is that hospitals and medical and dental clinics are the dirtiest places in the world.
On the contrary, they’re super clean. Believe me when I say that hygiene is the top priority of any hospital or medical and dental facility. After all, we make sure that any procedure that needs to be performed requires aseptic techniques. We observe protocols to the tiniest detail in keeping the hospital and clinic environment as clean as possible.
But hospital acquired infections are a different matter altogether. They occur among the immunocompromised, those that stay longer than expected, entertain guests (even if we have policies on guest restrictions, there are just some entitled patients) without screening who visits them. I recall once when I was making my rounds that there were more than 10 people in the room of a newborn patient. I couldn’t help but blurt out – “wow the whole barangay is in town”. Only to have one of the relatives reply, “oh, we’re just 1/8th of the family.”
But that’s a Filipino tradition that’s hard to let go. If you look at the arrival area in the airports, you have one truckload of welcomers who probably are waiting to get a “pasalubong” from the balikbayan or OFW relative who is arriving. Some with babies and oldies on a wheelchair in tow.
The same is true in the hospital setting. There are kids that run around on the hospital floors and despite my having to inform the guards, nurses or anyone else for that matter – they just need to sign a “waiver” – because we don’t want to perturb the guest relations system.
Now that most of I and my colleagues have returned to the clinic and tell our patients that we’re ready to see their children, the parents ask the question – is it safe? Duh?!?!!?
The risk would probably be between 2-4. And with your doctor wearing a PPE, most likely 0-2. You don’t know the extent we go through just to make sure that the procedures we provide is to make sure that not only YOU don’t get sick but that we don’t get sick because someone was not truthful enough!
The gatherings
Then there are the parties.
In my family alone, we’ve had three birthdays uncelebrated because of the quarantine. We were ribbing at the fact that it officially meant we’re not another year older this year because there was no official celebration.
But yes, the most difficult of all to manage would be a social gathering of friends and family because you’re celebrating an occasion. No matter how you put it, there will always be children and elderlies that will need to attend these events (for fear of being ostracized from the family later on and because it is a family tradition to have the whole caboodle invited to the event).
And because there is no way anyone can even police a private affair like this, the only answer to the question on risk level is that this is a definite 8-10, unless you have an intimate dinner with the immediate family that resides in the same place as everyone else then that risk is now 0-3.
Public transportation
Taking an Uber or Grab or a cab is always the safest option. Driving yourself to work (or ride sharing with one to four people if you’re in a car) is another great option. The trains, jeeps, buses, tricycles and motorcycle rides pose greater risks because of social distancing issues. Then there’s also the handling of money for fare payment. There are no beep cards for tricycles, buses, jeeps and motorcycle rides in the Philippines. Barter is done through cash exchange – which are really really infested with all forms of microorganisms.
Then there is the crowd that needs to get transported from point A to point B. Majority of the people get to work by public transportation. We know that the roads are congested enough with private vehicles. The public transportation is the Philippines is bad. Really bad. To make a handful of people go to work by opening up the economy without transportation is hell on earth.
In short, we just created a mob.
And whatever social distancing measure you try to apply, it’s every man for himself because by hook or by crook, their mantra is “ I owe I owe so off to work I go.” And nothing matters anymore when the stomach is empty. Not even COVID-19.
The risk level? 2-4 if it’s a private transportation or share riding app. Definitely 6-9 if it’s a public transportation system.
The workplace
Last but not the least is your work area. And I’m talking about offices here and not the other work spaces mentioned above.
Arrangements can be made requiring a subset of workers who report to the office on certain days of the week while spending the other days working from the confines of their home.
In the offices, during work hours, people are more often than not separated from each other. Working quietly in their desk or work space. It’s the break time gaps that allow a crowd to come together. It’s lonely to eat alone on your desk. Workers will always find the opportunity to converge in order to share stories and food during break time. And share the virus as well.
While difficult, gatherings in the pantry is highly discouraged. Eating alone is the rule so that there will be no food sharing as well. It cuts down conversation time, decreases gossip in the workplace, and increases productivity. Not to mention that those are just the bonuses from the primary goal of decreasing transmission of infection in the work environment.
—————
This is not an exhaustive list. And you can make your own. I’ve provided 5 essential points that you can use to assess the level of risk. And you just need to score them from 0-2 (0 – no risk, 1-intermediate risk, 2- high risk). Total them and you should get your answer to your question.