I have provided the link of the Department of Health’s Covid-19 tracker. There are various sources where one can obtain good data analytics from. If you go to this link, you will find out that the improvement in the COVID-19 tracker.
Then there’s the down side. The data analytics is wanting in useful information. The kind of information that should make us decide on how bad this Novel Coronavirus pandemic is in the Philippines and whether we’re actually “flattening the curve”.
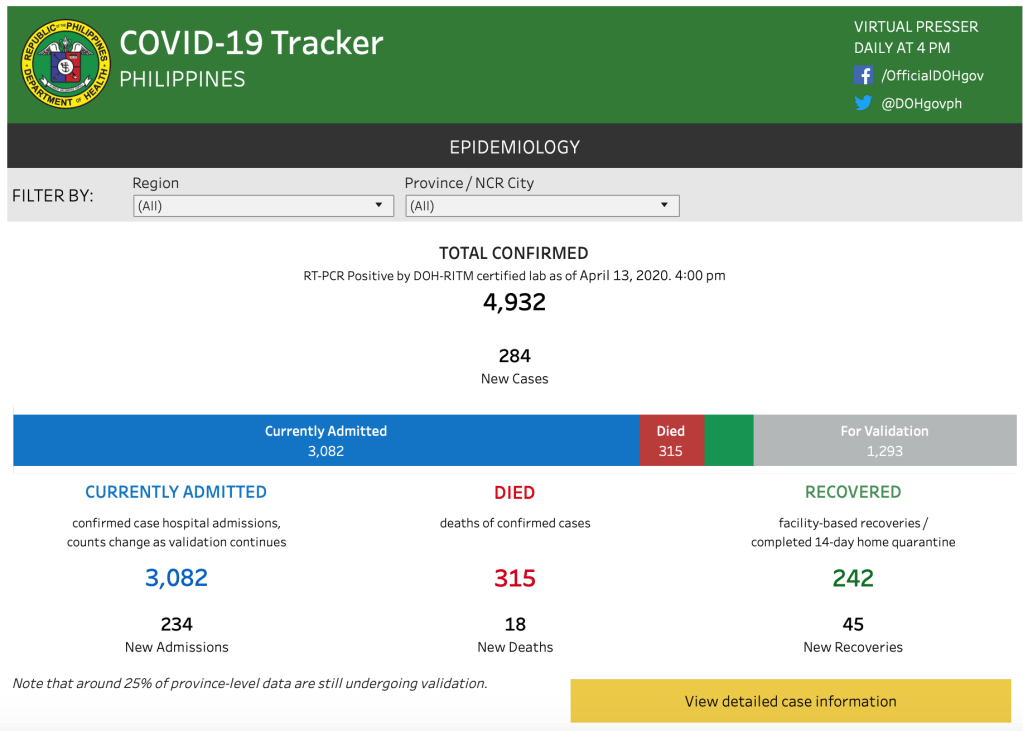
Once you get into the site, this is what you see.
It gives you a pretty good picture of the daily information on the epidemiology of COVID-19 in the country. 4,932 confirmed. 3082 currently admitted (they don’t identify how many are critically ill and the rest are probably mild and quarantined.) 315 died so far. 242 recovered. Then in the gray bar are the ones “for validation”. There’s a caveat that says that “around 25% of province-level data are still undergoing validation”. But wait…there’s more!
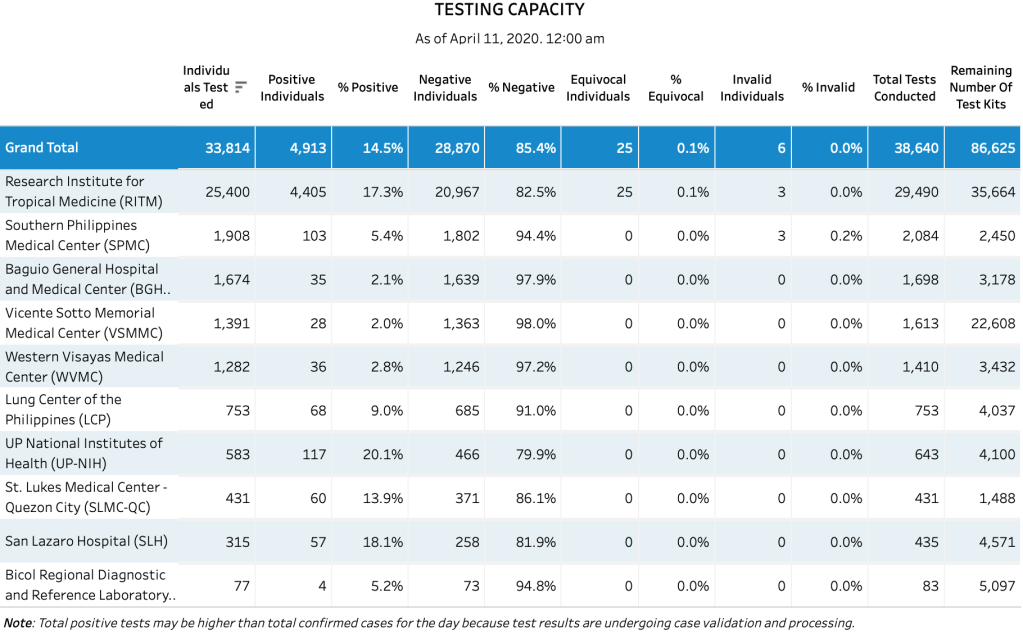
If you scroll down a bit, you will see the table on testing capacity. Here’s where the data actually differ. The testing capacity as of April 11, 2020 showed 4,913 positives. The total confirmed as of April 13, 2020 is 4,932. On April 11, the DOH officially reported 4,428 confirmed cases. What accounts for the discrepancies in the numbers coming from the agency?
The 1,293 case for validation (said to be province-level data) is confusing.
I would assume that province-level data would point to tests coming from Southern Philippines Medial Center, Baguio General Hospital, Vicente Sotto Memorial Medical Center, Western Visayas, and Bicol Regional Diagnostic Laboratory. If you total their positive cases, that would just be 204 positives from the provincial testing centers.
We can assume that some specimens were sent to Manila for analysis. How many were sent to Manila? These inconsistencies in the numbers makes one wonder if they just deduct the total cases from the remaining cases in order to arrive at the discrepancy?
Let’s look at the numbers again.
4932 total confirmed. 3082 currently admitted. 315 died. 242 recovered.
Assuming the numbers are correct, that’s 3639 cases (admitted currently, died and recovered). What are remaining 1,293 cases “undergoing validation”? What does undergoing validation mean?
First, if they’re still not yet validated they shouldn’t even be part of the total statistic.
Second, is why are the numbers in the provincial testing centers not tallying (202 from all the provincial testing sites vs 1293 cases at the national level)?
The third and most vital query is – does the DOH actually have data on the patients that tested positive but were sent home for quarantine? How many of them returned for retesting? When you look at the numbers – of 4932 confirmed only 3082 are currently admitted. Or 1850 cases distributed as follows: 315 deaths, 242 recovered and 1293 for validation(?).
Data integrity is important in the analysis of outcomes and planning of mitigation strategies. It is, after all, the basis of our life after April 30.
The new site, while providing information on cases, deaths, recoveries, is wanting in the type of severity of the illness. We all know that not all admitted cases are in the ICU or are critically ill.
If we scroll down a bit, there’s interesting information regarding the availability of beds and mechanical ventilators in various hospitals.
This above information above while helpful is disturbing. If you look at the ICU beds, only 391 beds (out of 1,085) are filled. The remaining 2/3 are unoccupied. There are more than 87.29% mechanical ventilators still available. Yet reports coming from various private hospitals are that they are filled to the brim and that the healthcare system is overwhelmed by the coronavirus infection that some hospitals had to turn away patients.
Based on the data provided in the DoH website, of the 3082 currently admitted, 391 are in the ICU (as of this writing). That means only 12.7% are critically ill (needing intensive care).
There are more deaths than daily recoveries among those currently admitted. The graph below is a screenshot of the new daily deaths and new daily recoveries on the website. Implying that of the 391 cases in the ICU, 315 have died. An 80% mortality rate when intubated or in intensive care.
Of the 3082 cases admitted in the hospital, assuming that only 391 are in the ICU, what happened to the remaining 2691? That’s the majority of the patients. Who happen to be mild or moderate and probably recover.
Finally, there’s the interpretation of the data.
Cumulative is the operative word in the presentation of data.
Which means that regardless of patients getting better or dying, the total cases is what you see. But in reality it is not. Minus the deaths and recoveries, we actually are tracking 4375 cases that are still active. The deaths and recoveries are considered closed.
The red herring here? The ones for validation. They form the inconsistent information that needs an explanation so that it is not misinterpreted.
I’ve always told my former students in biostatistics that all the numbers should have an explanation. It is imperative that data gathered is accurate, valid and not confusing to the reader. It is also important that all tables and graphs are reconcilable. Otherwise, any conclusion or decision that is made with this kind of data is confusing and simply leads to bad decisions in preparation and planning.
The bottom line of good solid data? The April 30 deadline.
…well, that’s wishful thinking. But let’s pretend it happens…
NUMBERS MATTER
We all know that the only reason for people in government to consider re-extending the extension are the “numbers”.
Larger number of cases. Longer recovery time from more critically ill patients. Poorer recovery rates. Increased doubling rates. These are the numbers and endpoints that matter from an epidemiological point of view. And because these numbers matter, we need a unified accurate data in order to predict whether we’re getting out of April 30 alive or not. The Department of Health has made an announcement that this is currently in the works and that perhaps the deadline they set on April 11 for syncing all data should be helpful to the decision makers on any exit plan.
It cannot be a mathematical modeling that is predicted based on several assumptions that are not constant. Mathematical modeling has its limitations, because while it incorporates available actual data, its accuracy depends on the number of actual data into the various incorporated variables. If the variables used in the prediction model are “constants” and “assumptions” as well, then the modeling accuracy is compromised. Hence, my caution in using modeling parameters because this virus does not recognize the variable nor the constants of a mathematical equation. It will behave the way it does. Unpredictably.
All data must be coming from the National Government. Seriously, it is difficult to make heads or tails with the discrepancies in data between the Local Government Units and that of the National Government (Department of Health). You get reports from LGUs that report more cases than what the National Government releases, while other LGUs report less cases. You actually have this feeling that you don’t know who’s actually running the show.
Let’s use one website: https://covid19stats.ph as reference for all discussions in my blog (unless otherwise I use a different reference). I think it’s a very good one considering that it provides both national and local government data as well as the global data. While it is not in real-time, it is updated at least before 4PM (Manila Time).
Figure 1
Figure 1 above shows the data as of yesterday. Note also that this website started with information on March 27 at a 803 cases, 54 deaths and 31 recoveries. In short, by March 30 (3 days later) we stood at 1546 cases, 78 deaths and 42 recoveries. A doubling rate of 3 days. Which means that on April 2 we should see more twice the number of cases we saw on March 30. Did we? Well almost. On April 2, we had a total of 2633 cases, 107 total deaths, and 51 total recoveries. Which moved the actual doubling rate now to around 3.3 days. If you used a constant mathematical model, you would have expected that by April 5, we would have more than 5200 cases, on April 8 more than 10,400 cases on April 11 more than 20,800 cases and so on and so forth. The slope (rise in numbers) would be steep. The casualties would rise disproportionately as well. Yet on April 5, the total cases was 3246; 3660 on April 6; 3764 on April 7; 3870 on April 8; and 4076 yesterday April 9. Note that the doubling time also became longer from 7 days to 10.76 days.
Doubling time is the number of days it will take confirmed cases to double and is based on the 7-day daily average growth rate. The other variable that’s important to look at is the daily growth rate. The lower the growth rate, the more contained the outbreak is. (Table 2 below)
Table 2
This is why accuracy in data is important. This is the first trigger that will decide on life after April 30, 2020.
As the growth rate slows down, and the doubling time is prolonged, there is no reason why there should be an extension of the ECQ.
TESTING MATTERS
The second trigger in determining whether we’re getting out of this lockdown alive on April 30 is the capacity of the testing centers in the country. The backlogs in reporting. The backlogs in printing out the results. The number of accredited centers. How many tests are done per day and all these numbers I mentioned – should have a denominator. Out of how many tests are the reported cases? This will give us a better grip on the the first trigger because they are co-existent. A backlog in reporting is bad data mining.
THE ECONOMIC AND OTHER HEALTH IMPACT
This is the third trigger. Regardless of data, talking about the disease versus jobs and the economy that has faltered is moot and academic. We all want to come out of this pandemic in one piece. No one wants to be a statistic. I’ve lost too many colleagues close to me to this virus. And yes, we’re all afraid of the unpredictability of this virus. As of this writing, there are several promising experimental treatment models that are being conducted – from the Japanese experimental antiviral Favipiravir (Avigan) developed by a subsidiary of Fujifilm to Hydroxychloroquine + Azithromycin +/- Tocilizumab to the recently US FDA approved protocol for convalescent plasma. We see some light at the end of the tunnel, but that’s a topic that I will discuss some other day when we have better and more reliable clinical trials are available. And then there is the promise of a vaccine on the horizon.
Which means that there’s a waiting period. We need to sit back and wait. The magic potion is not within our midst. But the economic backlash is hurting not only the country but the world as well. As to how long a hungry stomach can withstand the wait is a different story altogether.
INTERPRETING AND REPORTING CONSISTENCY
I cannot tell media how to report. Every media outlet will have its way of trying to grab the attention of the viewer. As the late Mr. Felix Bautista once taught us, the first line of your story is the most important. It is what will enthrall your readers to read on or ignore your writing.
But I can teach my readers how to interpret the data.
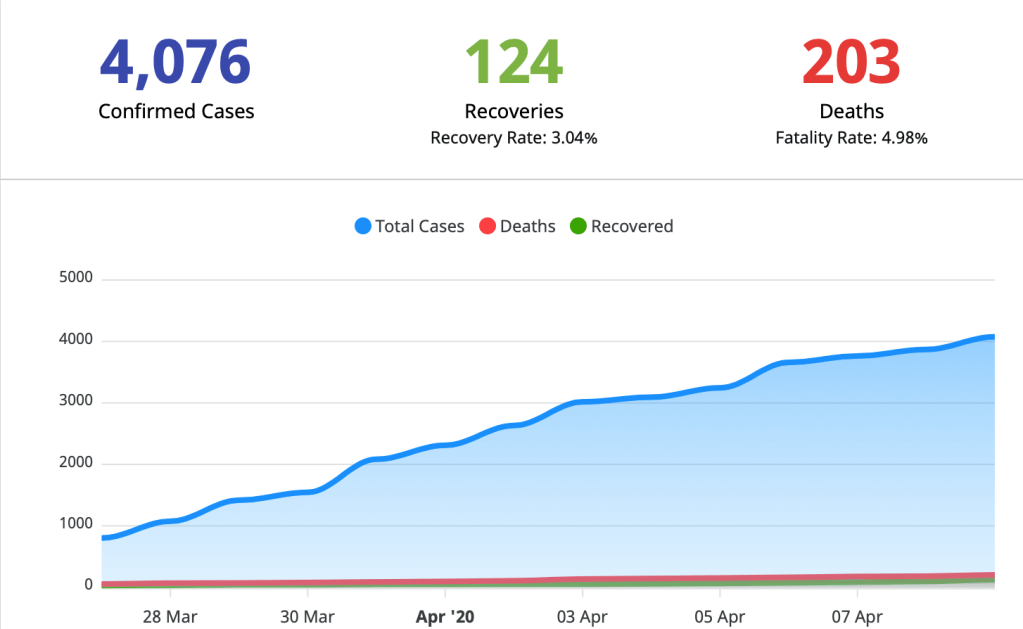
Figure 3
The data on Figure 3 shows you that we have 4,076 confirmed cases. I think what the media outlets should be reporting are the new cases. The 4,076 cases include all the cases since the beginning of when we were registering them. Again, if you look at the recoveries and deaths, these are closed cases. In short, of the 4,076 cases, 327 have had outcomes. They either died or recovered. In short, we’re just monitoring 3749 cases. And waiting for their outcomes.
We will not really know how many will recover (or die) until a few months when we’re seeing the trough of the curve.
Figure 4 above shows the data from China who had exited from their lockdown last April 8, 2020. They are still reporting new cases (in beige) and new deaths (in red) but their overall recovery is 77,455 cases (94.56% recovery rate), with 1,116 active cases remaining (no outcome yet, and 144 of them being in critical condition), and 3336 deaths (4.07% case fatality rate).
Their new cases are mostly foreigners or people who have returned from foreign travel.
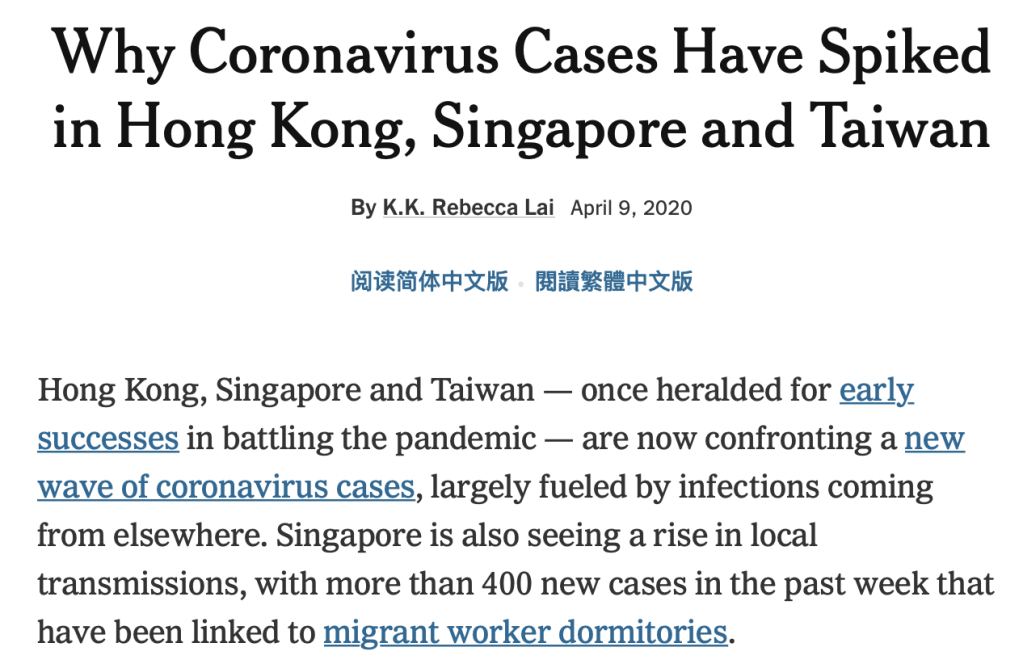
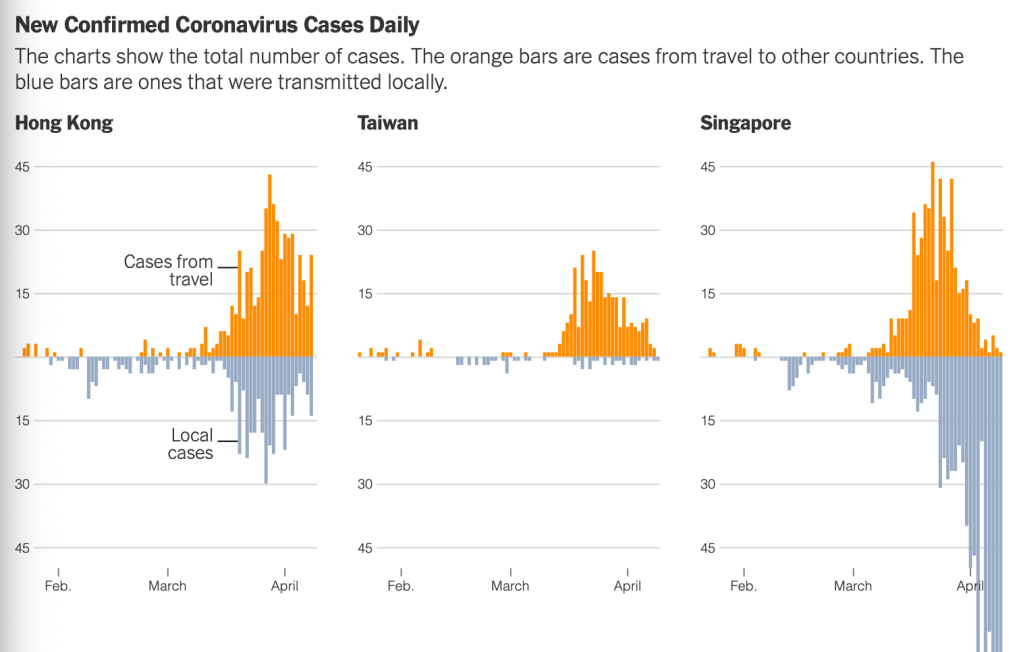
Figure 5 above shows the glaring data where there were so few cases after the lockdowns and a resurgence in cases after lifting it. Taiwan was hit most with the surge in new cases (orange bars) imported from other countries. Local transmission remains low. In HongKong, Singapore and Wuhan, the stories are similar, except that Singapore is reporting a surge in local transmissions.
Some normalcy should be brought back slowly. To ease the restrictions will require a concerted effort from every sector. Like a master conductor for a Philharmonic orchestra, he must be able to create a harmonious exit out of this lockdown.
Easing it will be the way to go.
Address the triggers. Set a deadline for the respective agencies. The deadline was yesterday. Obligate and hold responsible agencies that are part of the problem instead of being the solution.
Schools in the Philippines are literally jampacked. Online learning when applicable should be the mode for the rest of the remaining school year for college and graduate schools. Those in grade school should be made to stay home and allowed to move up in August. All schools should now be synchronized to open at at specific time. My suggestion – August 1, 2020.
Social distancing, hand washing, hygiene and wearing masks should be the new normal. Malls can slowly be opened (for essential goods) with strict social distancing and allowing people up to probably 1/4 the parking capacity of every mall. Restaurants can only operate if there are reservations made so that only half the capacity of the place is occupied at any one time. Take outs are encouraged. Drive throughs as well.
Hospitals should open its doors to NONCOVID patients. A triage should be in place at every hospital. Patients should be honest enough to disclose why they are there. Patients who fulfill the criteria as PUIs or PUMs should automatically seek medical consultation at a COVID designated facility. Hence, every private hospital should be encouraged to have a designated facility only for COVID patients separated from the rest of the hospital. This is so that other patients (which is the majority) that have other acute or chronic illnesses can be seen by the respective doctors. HMOs should put up their own facilities outside of the hospitals for COVID patients. For example, if you are a COVID-suspect, you can only be seen at the hospitals accredited by the HMO for COVID patients. This will partly address the issue of local transmission and contact with COVID patients. Remember, the majority of patients that require both elective and urgent care are NONCOVID patients.
There should be limitation of travel in and out of the various regions for the next 2-3 months in order to limit other sources of local transmission. Those who live outside of the NCR but work in the NCR should consider renting a place near their workplace for awhile. Regional travel can be reassessed after 2-3 months or earlier depending on the state of the pandemic.
Public transportation should be limited to the locality. Perhaps in order to avoid crowding, people who are unemployed or do not have work should not be allowed outside the homes in the meantime unless for essential errands (marketing or buying food). The type of transportation is important. Public transportation should only be filled to 1/2 its capacity.
Children and the elderly are encouraged to stay at home during this transition period.
Gigs, concerts, crowds, bars, night outs, movie houses, conventions, and other nonessential activities should remain cancelled until after the transition period is reassessed.
I cannot overemphasize the reintroduction of another wave after we have “flattened the curve”. The only way to sustain it is to close the borders into and outside of the Philippines in the meantime. This means that anyone who decides to travel outside of the Philippines or is a foreigner who wants to visit the Philippines will need to undergo BOTH of the following upon arrival: (1) PCR or rapid testing (2) mandatory quarantine for the next 14 days. If symptoms appear or patients test positive, they should be admitted to designated centers for PUIs and managed accordingly.
We should not overlook one other fact.
The flu season in the Philippines is the rainy season. That’s usually June. Encourage everyone to get flu shots. That’s one virus less that will complicate the management of any respiratory infection.
As the rainy season is around the corner, it would be disastrous that we’re going to be seeing a mix bag of infections – from dengue to flu – breaking out in the midst of an uncontrolled coronavirus pandemic.
I hope we get it right in the next two weeks. This is your best time the government can practice on what it intends to do after April 30. Seriously – we are left with no other option. Because life after April 30 must go on…
In a dazzling (dizzying) display of desperation (?), a visibly confused rambling of frustration on how to control the novel coronavirus pandemic and how it was affecting the dire economic resources of the Philippines was seen in the face of the president over a live announcement last night.
He didn’t mince words.
Behind all the garbles on afterthoughts from his trip to the toilet to urinate, asking the secretary of finance to generate money whether he steals or borrows, telling the people that there is a limit to what the government can offer and offering to sell Dewey Boulevard (so retro), asking for patience (which I am sure has run out of especially for the daily wage earners) because the virus has torn the very frail economy of this nation, and finally ending with the vast unknowns…I could understand his annoyance at the circumstances he’s in.
Huwag ka mahawa. Huwag ka lumabas ng bahay. Paano pagkain namin? Maghanap ka ng paraan.
Hindi ko alam kung [hanggang] kailan ko kayo sabihan. “bahay lang kayo”.
Hindi ko alam kung kailan ako makapaghatid ng pagkain sa lahat.
Hindi ko alam saan ako magkuha ng pera.
Hindi ko alam kung ano ang ipagbili ko. Kung may magbibili.
Hindi ito trabaho ng abogado. Trabaho ito ng medical experts, scientists. I just happened to be here. To my chagrin, bakit sa panahon ko tumama.
I end this with a prayer. Whatever be the correction – ang anomaly sa mundo. He created the world. And if God wants it ended, so be it. Salamat po.
The live telecast surely didn’t sit well with the audience.
It was not surprising then that after that exasperated moment, the announcement came this morning – the lockdown would be extended. Period.
The objective for extending it till the end of the month?
Let’s give people credit where credit is due. I actually see how hard the IATF (Inter Agency Task Force) is working trying to complete the arduous task of containing this global pandemic among our islands. As I’ve said in the past, in pandemic, some things will require decisive action immediately. Waiting for tomorrow is another day wasted.
And that’s what happened with the first ECQ and the night before the extension. The first lockdown sent people into a frenzy. Panic buying for the those who could afford. For those who had less in life, it was just pure panic. An exodus for the unemployed. A wait and see for those that are still holding on to jobs, which probably some will have none to return to when this crisis ends. The last three weeks was spent in prayer and hope. That life would be what it used to be on April 14.
I am sure that most (if not all of us) are glued to the daily numbers – new cases, new deaths, new recoveries. Media are quick to draw conclusions or confusions to the numerical values that are being churned out by the Department of Health. If you ask any grade school student to draw a graph based on the numbers culled the past 3 weeks, they’d tell you that there’s no consistency. And that’s probably because of the backlog in reports. The death of a 7 year old in the Ilocos region is a glaring example of how long it took for the results to come back. Five days after her death. And that’s just one case. How many more cases have had dismal reporting timelines? This is important because the management of patients (from treatment to contact tracing and quarantine measures of exposed individuals) highly matters on how quickly (and accurately) we get back the results and the number of people tested based on the released report. Moreover, accurate and timely data provides us the best picture on whether the lockdown is “flattening the curve”.
I understand the frustration of the president. I, too, share his frustration. And I’m a doctor already! When you can’t make heads or tails of the data, the frustration is real.
The first lockdown has shown us how much more work there is to do, and how unprepared we are at crisis management in a pandemic. Let’s face it, the only way this virus will ever go away is sadly – probably never. Even with the availability of vaccines for flu or any other disease, we’ve hardly eradicated many vaccine-preventable diseases except for smallpox in the last century. The search for a cure or treatment is at best for now, a trial and error method. A lot of theories and anecdotes, with little science (robust clinical trials) to back up various treatment regimens.
As a people, it’s only when we accept our shortcomings can we realize that there’s much more we don’t know. There are few short-term plans plotted out but a dire lack in medium- and long-term plans.
Those short-term plans are panned out at providing measly change for the poorest of the poor. The people who work in government are better taken care than those in the private sector. After all, no one will lose a job when you’re with the government unless there is no more government. How does the government plan to assist the private sector with respect to repayment and restructuring debts particularly for the micro, small and medium enterprises? Supplies purchased from large companies should be given a longer term grace period for payment rather than the original payment dates. But many multinational companies will not agree to this because they have employees to pay and their own needs to fill. While people in government are willing to take a cutback in salaries, are the people in the private sector willing to negotiate a 90 days payment option instead of 30 days for various goods? Mall tenants and other stall/store owners are in a similar situation. How many landlords are willing to forego rent to tenants who did not use the rented spaces due to the lockdown? These are just examples of incongruence in the “bayanihan” spirit of the Filipino people. The irony here is that it’s mostly these same people who provide donations in times of disaster as public relations promotions that are in disguise of being concerned with the poorest of the poor but take from the small and medium entrepreneurs. That is why I am not a believer of these corporations who give out “donations” yet don’t look after the smaller companies that keep them afloat. This domino effect, trickles down to the vendors and consumers in the end. And as the pandemic deepens, the economy will continue to falter to the point of collapse.
Then there’s the medium- and long-term goal. The idea of having designated centers for COVID cases in every local government is both doable and a good one. Remember, isolating infectious diseases and waiting out the course of illness until the patients recover on their own is the oldest method of containing an infection. Before the end of this week, every local government unit must be able to put up one. There are many unused edifices in the local government and placing their city health office in charge of such centers will free up the communities from having the cases monitored where they reside as well as the hospitals in having PUIs and PUMs occupy the necessary space for the hospital to operate regularly once more. People don’t know that there are more patients sick with other acute and chronic diseases who will require hospital care than COVID19 patients. Segregating the COVID19, PUIs and PUMs is vital in reducing the spread of the virus and thereby restoring some sense of normalcy in the community. It will also allow other sick patients without COVID19 to get better healthcare, and hopefully be at less risk or when they do get infected with SARSCOV2, be immunologically stronger at combatting this virus. Comorbidities that are well controlled have better outcomes than those that are not.
The real problem I see are actually the local government units. They’re like little kingdoms. There are those who have best practices. Then there are those who are a bit off not only in science but common sense as well. And that’s where the difficulty lies. There is no consistency in the implementation of recommendations. When the mantra is “every kingdom for itself”, it will be difficult to curb a pandemic of this proportion.
A long-term plan should also be discussed today. Not a week from now. Not after April 30. As the president mentioned, this is after all a battle. And a prolonged drawn out battle it will be. At the end of the war, only one will emerge victorious. Our fate depends on the strategist who put this plan together.
What do we do on April 30, 2020?
Is another extension in the horizon? And that’s the question that’s begging for an answer. I hope and pray not.
But I guess that depends on whether we’ve gotten our act together or not. At the rate we’re going, the plans the IATF have put forth should be strengthened and every LGU should abide by the general guidelines (if any) of the IATF. Additional local strategies must be in congruence with the general guidance provided by the IATF. Any local plan that deviates from the IATF should not be allowed. There should only be ONE agency responsible for the success OR failure of the mitigation efforts during the next 2 weeks extension period.
Allow some flexibility in mobility. We need to mobilize not only frontline workers but some other essential business establishments vital to the economy of Luzon (where the lockdown is limited to). Some form of public transportation should be restarted with conditions on how many to accommodate and the practice of social distancing. Trains and MRTs should not be operational yet. There should be no crowded places or events for quite awhile. Schools will be out probably till the upcoming school year but that’s the least of our problem because the kids will get their wish – long vacation – at last. To keep the crowd down, malls and bars and other recreational facilities should remain closed until such time that we have actually reached the lowest part of the flattened curve. Nonessential travel (both in and out of the country) should be avoided in the meantime.
We must set the expectations early on as we approach the deadline and prioritize the economy while taking into consideration the general health of our people (not only COVID19). Both the economy and health are inseparable in the equation of a healthy nation, with each of them being dependent on each other. We cannot care only for the COVID cases. There is a greater majority of patients who are sick with cancer, hypertension, diabetes, measles, dengue, hyperthyroidism, cardiovascular problems, COPD, etc. yet one case of COVID overwhelms a whole community and healthcare system.
In the spirit of transparency that there was a well-thought plan to begin with, the public should know the basis or criteria on when the lockdown can be lifted, the restrictions that remain after the lifting, and when and what to expect as we monitor the lifting in the next year or so.
Sadly, this is one virus that will never go away. It will have its peaks and troughs all year round. As doctors, we will probably look at every fever, sore throat, cough or colds and diarrhea in a different light from now on. The general public will not forget this pandemic for awhile. But for everyone’s sake (physically and mentally), we will need to get back to some sense of normalcy. That’s why we need to sing the song in the same tune now. And get our acts together in how to deal with this invisible invincible enemy in our midst.
I’m sure we are already at the edge of each others nerves. And for good reasons. When the norms of daily life are perturbed, it gets crazy. An unseen enemy. Unknown cure. A race against time. The number of cases rising. The death toll insurmountable. The last century alone, all the gains and accolades of medical science wiped away with one virus. A microscopic pathogen indisputably eroding governments, economies, and lives.
The battlefield in the hospitals are at a different level. We’ve never been more fearful of a disease as this. Every front liner is fearful for their lives but still serve the sick. In our communities, paranoia and fear has hit the core of every family – from the gated villages to the informal settlers surrounding them. But let me say this for the record and with certainty – the informal settlers have the least to lose here in terms of health and wealth. It’s the middle and upper class that are panicking. The poor, well, they’re just worried about their day to day existence. Work for daily wages, food on their table, a house over their heads. They don’t have bank deposits or stocks and investments and businesses to worry about. They’re used to what they have. All they worry about is a tad of health care, their grumbling stomachs, somewhere to lie down on after a weary day. Day in. Day out.
So my readers asked me one good question.
Will (or should) the lockdown be extended?
My disclosure is that what I write are based on all the data I can cull available for public access. Other “unpublished” or unreported information are factors that may change the opinion later on.
So here we go.
The answer is YES.
It should, however, be modified because we have now seen its promises, and gaps.
As the number of new cases rise (and it will rise because we have more testing kits now), the number of daily deaths will be the predictor of whether the lockdown is working or not. Let’s remember, the number of new cases IS NOT a reliable predictor of whether the lockdown of a community works or not because when the lockdown was declared, the number of cases were already on the uptrend.
Figure 1Figure 2
Figures 1 and 2 above show that the slope began toward the middle of March. I cannot overemphasize the fact the importance of testing here. It was an outbreak waiting to happen. We slept while the enemy was awake. Complacency and poor foresight. As long as we see those numbers go up for awhile, don’t expect the recoveries overnight. They won’t go down until 2-3 weeks from the time they went up. We started the steepest climb only last week. How steep will we go depends on multiple factors.
The good news is that if this lockdown did not happen, there would be more new cases and new deaths.
The bad news is that, as in all lockdowns, the lockdown came too late. By the time an outbreak has occurred or is recognized, the virus has already taken over a proportion of the population for it to spread. The R naught (R0) of SARS-COV2 is low. Scientists say it’s round 2-3. The R0 tells us the infectivity. For every case, 2-3 patients probably get infected with the virus. Compared to the seasonal flu where the R0 is around 1.3 or chickenpox virus where the R0 is 10 or measles virus where the R0 is 15. https://www.livescience.com/new-coronavirus-compare-with-flu.html
Why do these numbers matter? Because they are part of the basis in decision making for our exit strategies.
What works?
1. We know that physical distancing works. The less crowded the place is, the less infectivity rates are. That’s common sense.
2. Unlike the World Health Organization, I disagree that masks should not be worn. The WHO has flip flopped several times on various recommendations or whatever it recommends. They are, a political organization. They are not a regulatory agency. What may be effective in Uganda or the Philippines may not necessarily apply to Japan or the United States. Every country has its own vulnerable spot. And ours is relying on the WHO for an opinion. Their observations are noted. Do we need to follow it? No.
Masks should be provided and worn outside of the home, in public, when tending and seeing patients. The proper mask is also essential. Those washable porous masks that have Dora or whoever character etched all over don’t work. Wearing a mask should be the norm now. I cannot overemphasize how much a highly useful preventive equipment it is for many respiratory pathogens. The mere fact that SARS-COV2 is a respiratory virus, protecting your face with a barrier is just common sense.
3. The surge of OFWs returning home is scary. Not that we don’t want them home. We do. What do we do when they get here? More than anything, they must all be swabbed. Their absence of signs and symptoms, fever or other factors ARE NOT reliable. Majority of our patients do not reveal a history of travel. Travel has become a stigma suddenly. We learned that with the death of a doctor from a patient who lied. The patient had a travel history. Got sick. Got people infected. Didn’t tell the truth. And a doctor died. Where’s the fairness in that? Swab them all. Quarantine them for 21 days. For patients that are positive, they need to have 1-2 negative swabs depending on the clinical status of the patients on discharge. Patients that develop symptoms and are critically ill must have 2 negative swabs before being discharge. And its not only the OFWs. Even those that have arrived in the Philippines in the last 30 days should get swabbed. The Department of Foreign Affairs and the Bureau of Immigration surely has a list of all these people who have arrived. They should look for the travelers and swab and quarantine them until all results are available.
4. PUIs with mild symptoms should be segregated and admitted to a facility only for PUIs. They must not be allowed to be part of the home or community. This is to make sure that they are not violating any quarantine measures. You know how ingenious the Filipinos are. Segregating them will minimize having a total lockdown in the communities.
5. All PUMs should be monitored properly. There are many ways that the local governments and barangays can assist. The identities of these patients can be provided and the data privacy act can and should be waived under these extreme circumstances , otherwise we end up in a catastrophe. The barangay can monitor the household 2-3 x a day. Everyone in the household should isolate the PUM in one room dedicated for the patient. Protocols are in place for self-quarantine. For the informal settlers or those that have no dedicated room for PUMs, the government should be able to provide makeshift places for these. Tap the public and private schools which are currently closed. PUMs have no signs and symptoms and will need very little monitoring except for food, water, shelter and keeping them locked in a room for the next 14 days.
6. Malls, stores, movie houses, bars, offices and restaurants should remain closed until May 3, 2020. We can reassess later the situation. Restaurants can serve take out food only but no dine in. Businesses that can work from home should be encouraged to work from home until May 3. Businesses that will need physical presence of workers should have a minimum work force or skeletal schedule so that it is not packed.
7. Curfew should remain in place from 9pm-5am every single day. This will minimize movements in any community.
8. Schools should remain closed until the end of May. The highest transmission of a virus will always be a crowded environment and believe me when I say that the physical distancing is least observed in pediatrics.
9. All children and the elderly (> 60 or 65 years old) should stay at home as much as possible. Unnecessary travel should be avoided among this group.
10. Public transportation should be limited. Jeepneys and Buses and Taxis can be allowed but the number of passengers should be limited. No tricycles or bike riding apps should be allowed. Trains and MRT/LRT should not be allowed until such time that we have seen flattening of the curve.
11. Every region must have its own accredited testing center before you can even consider lifting or modifying the lockdown. We need to capacitate every region because the delayed results due to backlogs are deadly. Some patients will present in an unusual manner. By the time you get the results, some of them can end up infecting 2-3 patients who in turn have infected 2-3 more people and so on down the line depending on the day the results come out! Without this being in place, you cannot lift the lockdown OUTSIDE of the National Capital Region.
12. The Bureau of Immigration and Department of Health need to work together and we cannot rely on patient information. Every patient that is a PUI, PUM, positive (dead or alive) should be verified with the BI for a travel history – when, where, and what aircraft? This is for documentation and contact tracing purposes. Contact tracing is much easier when the patients are truthful with their information.
These are all common sense. They will work. If our government officials can work together. It’s disappointing that there are government agencies that create issues that are divisive in times of crisis so that they can lick the ass of people in power. Hey – this pandemic is about all of us, not about your political future. Get a grip on reality! If and when we all get out of this alive in the next few months, believe me, it will be payback time. Accountability among the government officials shall be made. And those that stole, corrupted, abused, and conspired evil during this pandemic should be held responsible for the outcome.
So yes. The lockdown should stay unless these issues are addressed. Then we can work on a week to week basis on how we can go back to our “normal” lives. In the meantime, this will be our new normal.
Oh before I end, the kit is still the most important tool we have here. I started blogging about this virus way back in January. It started with one simple article entitled “Pandemonium”. The rest is history.
How we tell the story, who we listen to and how factual the information is, and how it impacts on peoples lives and futures – that’s what matters. Let’s hope and pray that this government has an exit plan. Not one out of ranting but one that is well thought of. Because you accepted the role to lead, you have no choice but to lead us out of this pandemic with the least casualties.
We have only two scenarios as we approach the April 12 deadline of the Luzon Lockdown period.
It either gets extended a few weeks more or it gets lifted.
Either way, the bottom line is not only the human toll this pandemic is causing but the economic toll as well.
COVID-19 has changed the paradigm of what is the “new normal”. The millennials and the more recent “alphabet” Generations have never seen anything like this. Neither have we.
Two scenarios will play out as we go towards the end of the second week of being “locked down”.
Let’s be realistic. The number of new cases (and sadly new deaths) WILL NOT go down overnight. Or soon, for that matter. So let’s keep our expectations real. Locking down everyone for the next month will not make the statistics decline NOW. Remember, it took China in general and Hubei in particular almost 3 months to bring their numbers to where it is today. But they had a different model. And isolating Wuhan from the rest of China and the rest of the world took an economic toll on the country. But China will always be China. They are, after all, an economic powerhouse. They can build a hospital dedicated to managing SARS or COVID-19 in a matter of 10 days.
Keeping it real, the Philippines will always be the Philippines. The eternal beggar for donations. Let me call a spade a spade. We recognized this problem early in January. There was one death in three cases. From a foreigner who traveled from Wuhan, China to the Philippines via Cebu into Dumaguete and finally into Manila. He later passed away in a government hospital. That alone should have served as a red flag.
How we even got from that point to where we are today is a different story altogether. But the answer partially lies in what President Duterte said – The Kit is the Kit.
BEST CASE SCENARIO
The 4-week lockdown will hopefully slowly bring the number of positive cases down in the remaining 2 weeks. By “containing” everyone and presuming everyone is positive for the infection or are potential carriers (note: asymptomatic), we make the viral “infection” run its normal course. People within the same household who probably have mild to no infection will recover on their own. If enforced properly, this will curtail ongoing community transmission. Those that progress to being critically ill are then hospitalized, isolated and hopefully, recover with minimal sequelae.
The numbers should gradually slow down. The “curve” will flatten. The limited healthcare resources will not be usurped. And perhaps in another two months, life will breath new air.
WORST CASE SCENARIO
Then again, the success of a lockdown is a hypothetical presumption. It may work best for highly disciplined countries. Those with very few informal settlers. Those with better healthcare resources. And those with best economies because they have the means to feed and fend for its people. Like a zombie movie out of Netflix, the gated communities will probably be the last or least affected because they have the most resources.
How long do we lockdown and what are our grounds for endpoints? The anatomy of disappointment are expectations. As we near the date, are we seeing what we want to see? Why or why not? Should we extend the lockdown? If we do, how long do we extend?
Metro Manila is a highly dense city. We have more people here than Wuhan alone. More than 15% of people in the Philippines residing in Metro Manila. While there are many gated communities in the metro, they comprise only 1/3 of the population. Majority are informal settlers. How to quarantine a family of 10 that live in a 15 square meter area or a community whose homes are a thin plywood board apart with access alleys measuring 1 meter in width is a virtual nightmare.
So, yes. We need to get out of this lockdown in the next few weeks. Extending it is an option but a calculated risk on the economy of a third world nation like ours. As the poor would say, they will not die of Coronavirus but of hunger. We cannot keep giving them dole outs. Micro, small and medium enterprises will eventually crumble, with the smallest losing the most and most likely will be unable to recover at all. People will lose their jobs as these owners will need time to recuperate losses. Half of them will not be able to bounce back. The remaining half will struggle against the tide. There will be massive lay offs. Riots, violence, looting, unrest are worse case scenarios.
Is the lockdown the only solution?
No. And we need to get out of this rut quickly while taking into account the lessons learned from how other countries are managing their own crisis.
That’s why we need a plan B. This government should learn to shift gears now by appointing experts who understand crisis management and not rely on amateurs who only have political clout as the qualification for being appointed into public office. Sadly, some Filipino politicians use any form of crisis or disaster to be able to tap into government funds for their personal gain. Greed, power, and ambition are well entrenched in the DNA of corrupt politicians who run for public office because to them, it is a business enterprise. For a country like ours, it is a family affair.
As the various cities and provinces move into lockdown mode, the longer the time to relief, the more the economy will take the brunt of the pandemic. It has hurt more affluent nations already. Imagine the impact it will create in a small country like ours whose financial reserves are being depleted to sustain the fledgling business sector and the jobless.
The cash assistance program of the government IS THE WRONG solution to the current crisis. It is not a sustainable solution. The small patches being addressed include giving cash assistance to the informal settlers and those unemployed due to the crisis. Which I personally think is a bad idea. This is a problem that will last into Plan B. Which means that the government will need to sustain the micro, small and medium enterprises in a time of difficulty. They will need to give up more than just dole outs to the poor. The question is, are they willing to?
This would mean not collecting taxes, SSS, Pag-Ibig, Philhealth, GSIS and other contributions for an agreed period of time. This would also mean that losses can be claimed against taxes. Loan reprieve should not be voluntary but mandatory. All banks and other lending agencies should be mandated to require those who have existing loans if they wish to restructure their loans to lower rates. It is unfair that current lending rates have been lowered but not adjusted for those whose loans are locked in at a fixed rate at a time when they borrowed money from them. Those who are willing to hold off payment for say, 3 months, should be allowed to do so in order to recoup the financial losses of this lockdown. Local governments should be mandated to provide a reprieve to local businesses as well. Rebates in business permits can be given. For example, for those that pay quarterly instead of annually, the second quarter payments should be waived. While the business permit may be based on the gross income of the company in the year before, it should be able to assist the local business sector these unexpected extraordinary losses. In addition, it should be fair in next year’s assessment when paying for a mayors permit. (I am sure everyone knows that the LGUs turn a blind eye when it comes to the business permits. They will not believe the income tax statements you declare and insist their own computations.) Reprieve from rental of business establishments where the offices or stalls or stores in malls should be granted as per duration of the lockdown. In short, greed must be tempered from all sectors.
Sustaining the smaller and medium enterprises is essential. The aftermath of the pandemic will impact not only on health and lives of everyone but on the economic repercussions of the lockdowns. Let us face it, at the end of the day, it is those who have the least in life that suffer the most. If these small and medium enterprises close, there will no jobs to go back to. And everyone loses.
PLAN B
There are two models that can be used. The China experience (total lockdown) or the South Korea experience (no lockdown at all). The people in the government can integrate the experience of both countries and perhaps create a hybrid one for the Philippines. Using either of models (China or South Korea) ALONE will not work because our economic structure is fragile and poor.
The article points that the lessons, “while hardly easy, appear relatively straightforward and affordable: swift action, widespread testing and contact tracing, and critical support from citizens.” The four lessons are:
Lesson 1: Intervene Fast, Before It’s a Crisis
We were there in the beginning of this war. Three cases all foreigners. One death among them. Then we were stumped. Too few testing kits were at our disposal. Even up to today, we’re stuck with the bureaucratic red tape and the parasites and opportunists who take advantage of their positions in government to overtake the queue or by-pass the algorithm on who we prioritize for testing.
We intervened ahead of the world. Our major mistake was the mixed messages being sent by various agencies. Basic epidemiology would have taught us that if there was 1 death in 3 cases, the overall case fatality rate is 33% for the country. A number far too high from the average case fatality rate of 4-5%. Which means we were not picking up the real numbers. To have one casualty from the virus, you needed to find at least 25 cases.
But the virus has arrived. And the traditional response may not be the solution here.
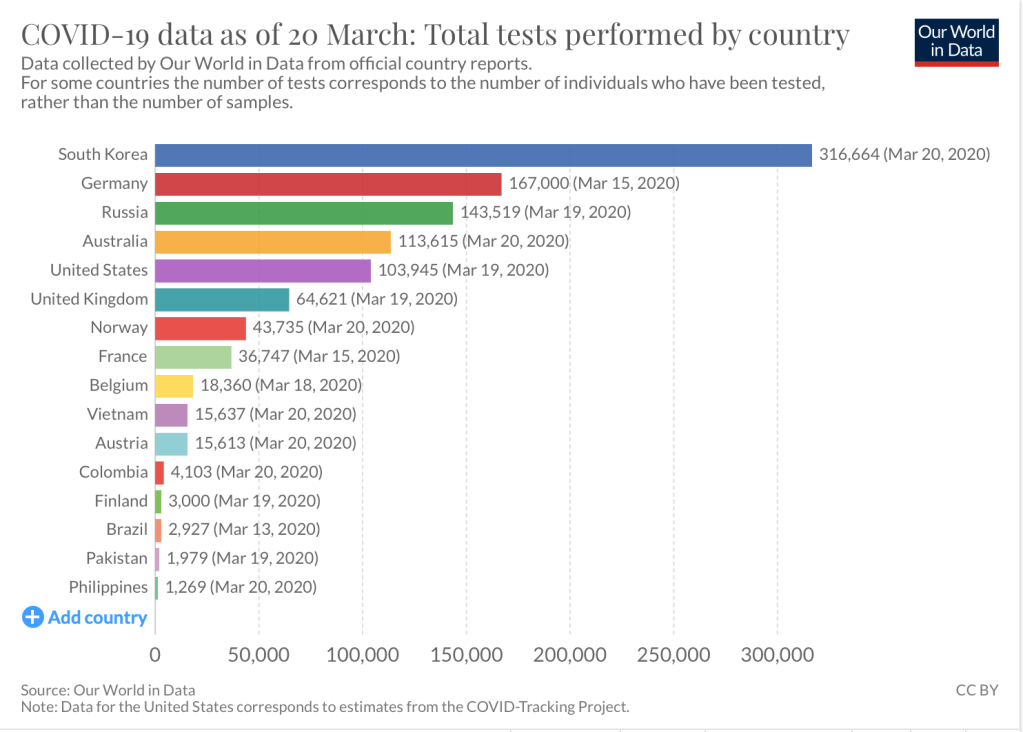
Culled data as of March 20 shows how far behind we are when it comes to testing. As the kits came in last week, the numbers began to swell. Everyone wanted to get tested. Understanding testing is vital in the decision on whether we test those at risk, those exposed, those at highest risk and/or test everyone?
But should we test everyone?
No. That would be a waste of resources. And may provide a false sense of security.
Like any laboratory test – reliability and accuracy is crucial. The tests should be be done in a safe place by well trained people who pass accredited and quality standards. In a nutshell, the validity of a testing kit will need to get verified. Results can vary between 30-60% accuracy. Other reports include 10-30% pick up rate depending on what you use. And are dependent on the timing, how the specimen was obtained and transferred, the severity of illness, the viral load and of course the way the specimen is run in the laboratory. These factors alone will make testing in a country with 7,641 islands a strategic impossibility.
The model used in Korea is opening more testing centers. The question is – do we have enough testing centers that fulfill the requirements for biosafety in handling specimens for these tests – in the country? The answer is a NO. Even if we beef up capacity, it will take months before we can have enough accredited laboratories for testing along.
To show you the model of South Korea, here is what they did:
This is most unlikely easy to put up in the Philippines. Hygiene, the very basic tenet of infectious disease is difficult to enforce in a community that lacks water, basic toilet facilities, and garbage disposal. Ignorance is also important to manage, doctors included.
What can we do realizing these limitations?
After the curve sees some flattening (which won’t be anytime tomorrow), mitigating the spread is vital. The key is to do testing on EVERY SUSPECTED CASE (not on everyone). This way we can conserve resources. All patients who are positive, regardless of severity of symptoms should be admitted to a designated COVID facility. Since schools have been closed, public or private schools can be used as COVID facilities for those that DO NOT have severe symptoms that will require hospital care. Food, water, and isolation is all that is needed. Making them stay AT HOME in the community will place more people at risk. Knowing the Filipino mentality and culture, home quarantine will not work.
Lesson 3: Contact Tracing, Isolation, and Surveillance
The Department of Health through their Epidemiology Bureau does a lot of contact tracing. The challenge is the patient. Some (if not many) of whom are afraid to reveal they have come in contact with patients for fear of being positive for the virus and the idea of being isolated. In short, people must be willing to lose a part of their privacy as a necessary trade-off for the good of the community.
Here is the model used in South Korea:
For all the technological wizardry of this nation, and how socially connected Filipinos are with their gadgets and other platforms, creating an app similar to this is a walk in the park. Two large telcos – Globe and Smart – should be mandated to work with the government in providing free data to those who will eventually need to use this app during self-quarantine.
Lesson 4: Enlist the Public’s Help
And this is where it gets a bit tricky.
Our bayanihan spirit defines us as Filipino race. But sadly that same spirit isn’t a consistent one. When people do things in order to be recognized as heroes in the end, we all end up as losers. Finding recognition at the heart of an outbreak of this proportion is not a solution. It is a problem. While government needs to listen to suggestions from private sectors, the private sectors should be able to sit down and work with the government on various matters. For example, certain corporations can help at procurement of PPEs and face masks (eg. banks and other lending institutions), while others focus on their special fields (telecommunications, food manufacturing, etc). We don’t ALL have to donate food. Equipments, health facilities, testing kits, disinfectants, etc are at the core of lacking in support. Let’s segregate it. And it would be fantastic if we had only ONE keeper of funds for the private sector donations that would turn it over and do accounting with ONE recipient of funds from the government sector (perhaps the Department of Finance). This way, accountability is transparent.
LIGHT AT THE END OF THE TUNNEL
Either way, the virus will disappear slowly.
Will it ever go away?
Scientifically speaking – No.
At best, after the dust has settled, we will understand how to recognize early this disease, manage the infection and hopefully find a treatment, and discover a vaccine.
The next two weeks will be crucial. It will be a defining moment on whether we proceed to doing mop up operations after the war or prolong the war. This invisible enemy in our midst is so far winning the war. A measly virus that has claimed lives, disrupted economies, changed the normal way we live and breath and engage with families and friends has the upper hand now because we hid under the rug the red flag two months ago when a foreigner died of COVID19 in our country.
The perpetual beggar stance of our nation is disappointing. We have billions to spend on intelligence resources, private planes and foreign travel and yet we wait for donations for – THE KIT.
The next two weeks is crucial. We either have plan B or the virus continues to decimate us medically and economically.
This government can have its most defining moment now or be the ultimate lackey because no one will ever forget this pandemic that will forever be etched in the history of science and economics. Ever.
Life in the metro, and in most parts of the world, has drastically changed in the past few days. As more new cases of the novel coronavirus are being reported, some people seem to be losing it. Literally, jumping the gun and going gaga over the additional cases that are being reported.
Epidemiologist, Adam Kucharski in his book “The Rules of Contagion: Why Things Spread and Why They Stop” proposes an interesting perspective on this topic during this lockdown period.
Li, Pei, et al. in Science (16 March 2020) published an article https://science.sciencemag.org/content/early/2020/03/13/science.abb3221 analyzing the prevalence and contagiousness of UNDOCUMENTED novel coronavirus (SARS-CoV2) infections is “critical for understanding the overall prevalence and pandemic potential of this disease.” That publication (which serves as an interesting read) estimated that 86% of all infections were undocumented before travel restrictions were imposed in China on January 23, 2020. “Per person, the transmission rate of undocumented infections was 55% of documented infection, yet due to their greater numbers, undocumented infections were the infection source for 79% of documented cases. These findings explain the rapid geographic spreads of SARS-CoV2 and indicate containment of this virus will be particularly challenging.”
The study indicated that multiple factors including: identical and isolation of undocumented infections, awareness among health care providers, availability of viral identification assays, use of face masks, restricted travel, delayed school reopening and isolation of suspected persons can potentially slow the spread of the disease. Combination measures increase the reporting rates, reduce the proportion of undocumented infections and decrease the growth and spread of infection.
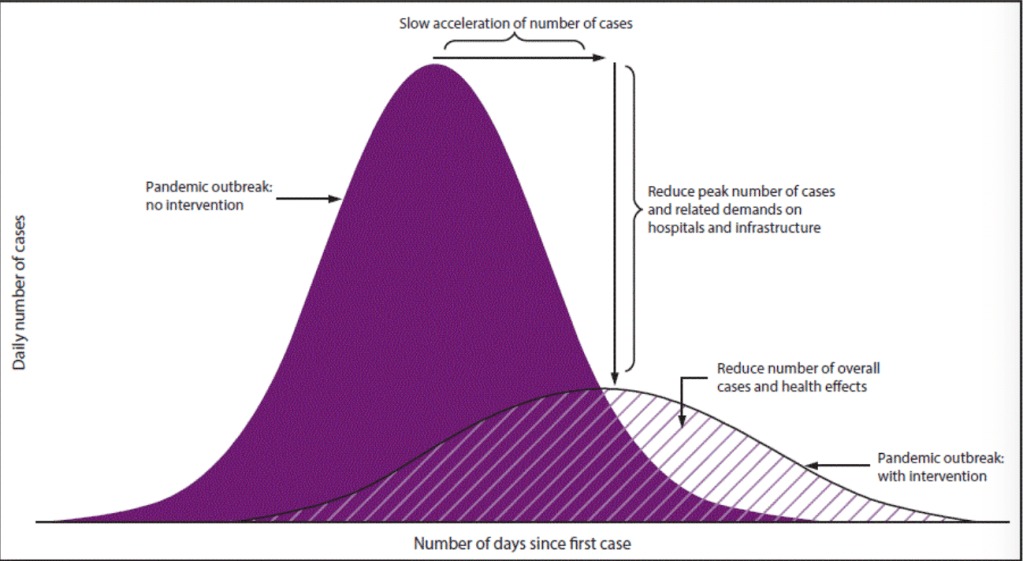
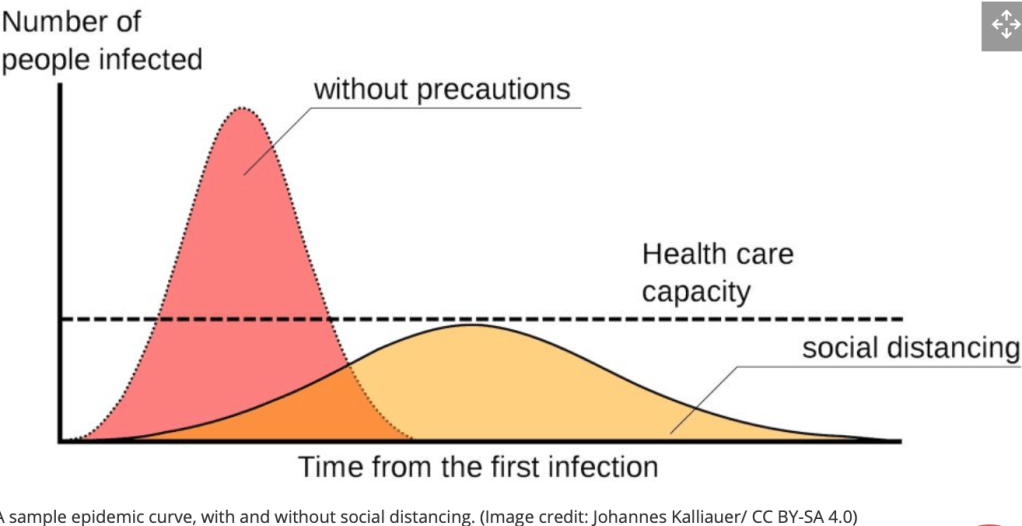
The lessons learned from the outbreak of the novel Coronavirus in Wuhan is a bitter pill to swallow for the global community. Experts in epidemiology talk about “flattening the curve” in order to primarily slow down the acceleration of number of cases. By slowing down the case rates, the burden and demands on various resources of the healthcare system is indirectly addressed. https://www.livescience.com/coronavirus-flatten-the-curve.html
Without intervention during a pandemic outbreak, the number of cases continue to rise, significantly overwhelming the healthcare system. Temporary intervention measures include lockdowns, quarantines, isolation and social distancing. It reduces the peak number of cases thereby reducing the number of overall cases. A disease declared as a pandemic will take years to eradicate. The discovery of vaccines may provide the long-term solution but it is not something that will occur overnight.
A pandemic will take time to naturally “flatten” on its own. Because of the initial overwhelming burden on scarce resources of healthcare (especially in third world countries), the death toll will be much higher. Those at the forefront are primarily affected. If there are less healthcare workers to tend to more sick people, the mortality and morbidity rate increases. If there are more sick people that will need hospital beds and ventilators because of more severe COVID-19 infection, the already limited resources are usurped more quickly. Scales of outcomes then become dependent on financial capacity for better and more aggressive care.
In epidemiology, the idea of slowing a virus’ spread so that fewer people need to seek treatment at any given time is known as “flattening the curve”. It explains why so many countries are implementing “social distancing” guidelines.
Brandon Specktor, Coronavirus: What is ‘flattening the curve,’ and will it work?, LiveScience, March 17, 2020
The broken lines represent the health care capacity of a country.
In the above graph, as the number of people disproportionately increase and no precautions are placed, the health care capacity is exceeded, exhausted and fails. In order to maximize (not overwhelm) the health care capacity, there is a need to slow down the infection rate. Flattening the curve assumes that the same number of people ultimately get infected, but over a longer period of time.
Does it work?
In 1918, a global pandemic of Spanish flu was seen. Compare two U.S. cities – Philadelphia and St. Louis. Infectious disease experts warned of the flu spreading in communities. The reaction of both communities was different. A massive parade went as scheduled in Philadelphia, gathering hundreds of thousands of people together. In 2-3 days, thousands of people in the Philadelphia region started to die. At the end of six month, 16,000 deaths were recorded. In St. Louis on the other hand, the city officials implemented social isolation methods – schools were closed, travel was limited, personal hygiene and social distancing was encouraged. At the end of six months, 2,000 deaths were recorded – 1/8 the number in Philadelphia.
How long is this going to last?
That’s the question that’s begging for an answer.
Unlike 1918, we’re living in a different era. More than a century later, our tools at combatting infectious diseases are more rapid, accurate, and precise. But even cutting edge technology and digital advancement won’t solve this problem overnight. One avenue science has not caught up with is a contagion unknown by all. When the enemy is new, the learning curve is steep. Which means that it will take in casualties before we know how to deal with it.
This will not go away anytime soon. With appropriate mitigation measures – both medium- and long-term – we will be able to suppress this. We need to bring the number of reported cases down using ancient aggressive epidemiological tools – social distancing, quarantine, lockdown of high risk communities, and testing patients. Belligerent testing, case finding, contract tracing are vital to keep the cases declining. When the dust finally settles, the government should put into place an overlapping long-term plan on how to keep the numbers down. For example: (1) all people who travel should have mandatory quarantine of a minimum of 14 days upon arrival. (2) Everyone who comes in contact with a COVID-19 positive patient, should undergo testing, monitoring and self-quarantine regardless of test status (if any). (3) Social distancing should be norm for the next few month until this blows off. (4) Schools may need to get cancelled for the rest of the school year. (5) Vaccine-preventable diseases should be mandatory for all so that we are not taken aback when another outbreak (preventable at that) surprises us in the future. (6) Honesty is a direly lacking trait among Filipinos. For more personal reasons for that matter. (7) Sale and events that will entice a crowded group should be canceled up to the year end. But these are just examples and I am sure people will get upset to some degree.
Eradication is another story altogether.
Someone asked me if this will ever go away. The answer is no. I don’t think so. One strategy to making this vanish is to develop a vaccine at best. But like any new drug, this isn’t like some Avenger movie where a vaccine is developed in a couple of hours, needle plunged into the arm, and presto – we’re immune! This will take quite awhile because whatever is developed out there needs to get tested for safety and efficacy. How long will it protect you? Do you need added doses? What’s the immune response to the vaccine? What are the short and long-term side effects? We all want to be guinea pigs during a crisis.
Let me end this by saying that it’s okay to be disappointed with what’s happening. Sadly, we still have a lot to learn about this virus. And how it will play out. The worst will spare many of us. But only resilience will make us survive this pandemic. Yup. The pandemic will end. As it did with the Spanish Flu of 1918, it ended in 1920. With the novel coronavirus, “what we don’t yet know is when.”
These are words that are unheard of in the last century in democratic countries.
In the context of a health setting, these words were last used in a flu pandemic in 1918. More than a century ago.
A hundred years later, who would have ever imagined that another pandemic would arise? Yet it did. The virus is called SARS-COV-2. The disease – COVID-19.
The coronavirus outbreak has harmed communities and disrupted economic activity in many countries
The New York Times 3.16.2020
The evolution of digital technology, social media and the internet has undoubtedly changed the way we live in the 21st century. Everything is now readily accessed by our fingertips. Mobile devices and other accessory gadgets have created wonders at how staying connected we can still be in spite this health crisis we’re experiencing. All these have cemented the fact that human beings are social creatures. It has become our core DNA.
However, when social distancing becomes the rule, our norms are perturbed. Daily habits get changed. Schools are closed. Mobility is restricted. Travel bans and vacations are at a standstill. Work is muddled. Deadlines and targets affected. Economies are tested. Finances are disrupted. Those that have the least in life, end up suffering the most.
Life is at pause mode.
In societies where life plays out on the street or in the cafe, where friends are greeted with kisses on the cheeks, the outbreak is creating fear and fragmentation.
Steven Erlanger, The New York Times, 3.16.2020
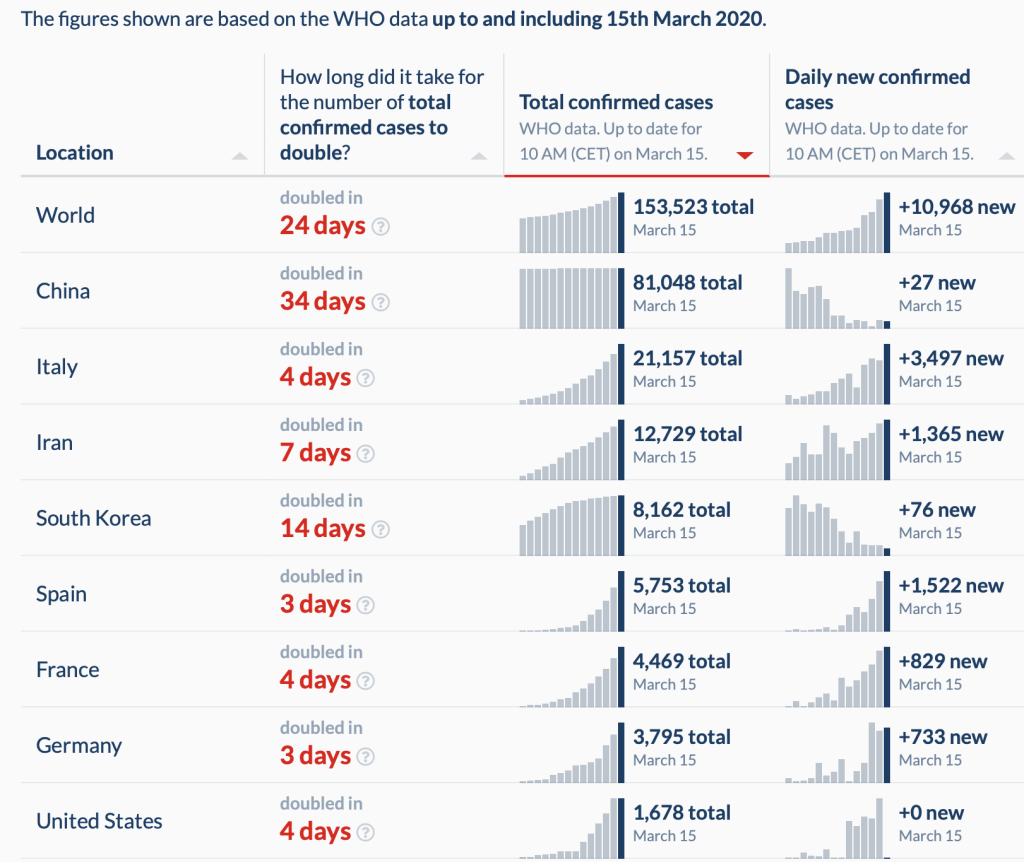
While the novel coronavirus gains steam outside of China and at a pace much faster than its spread in Wuhan, the doubling rates in the rest of the world has become a major concern.
In the above table it shows that aggressive testing is proportional to the doubling rate. The more aggressive we test on a broader scale, the longer the period to doubling time. Below is the Philippines data.
That doubling time is why we react the way we do now. The number of deaths has disproportionally risen. In one of my blog posts https://wordpress.com/block-editor/post/relativejoyforyou.wordpress.com/6568, there’s a daily track on the status of the pandemic. The stance of the World Health Organization at the beginning of this COVID-19 outbreak was a feeble one. That’s how we got to where we are today. The reactionary attitude of individual nations is rationalized. Albeit a bit late, they’re doing all they can to bring this pandemic to its knees.
So I’m writing this blog on a day off from the hospital because I am heeding the call of the government – stay home, stay safe.
Yet I cannot help but think about the other people outside my gated community. 90% of those that own businesses in Metro Manila are micro enterprises (not even small or medium). They invest their hard earned money in tiny businesses inside malls. With the shut down of malls or other places of business, they have nothing at all. Suffering an economic loss is an understatement. 80% of employees depend on the flailing public transportation system of the metro. No matter how difficult life is, how far they live, they will trek to their place of work because they have mouths to feed and bills to pay. The disruption in daily life is most lamentable among those who have the least in life. And so yeah, I’m not all rah-rah about the total expanded community quarantine, a.k.a, lockdown. That’s because the government forgot to think about the larger group of people affected by this lockdown. And when you have government officials who tell you to just shut up and shove it, well that’s the kind of empathy you get from people who have water for brains. We silently concurred with government people who were out-of-touch with reality because we have the means to sit back, relax and watch how this eventually evolves.
Then there are my colleagues who are at the forefront of the battle against this pandemic continue to tend to patients who flock to the Emergency Room demanding for tests because of paranoia or probably real COVID-19 illness. And those of us who still get up in the day and see sick and well patients because we are morally and ethically bound by the responsibility of our profession. The whole health force at risk, tired, undermanned and yet end up unappreciated by others who have nothing better to say or do because all they care about are their personal bravados.
I would least care for the generation that thrives on bars, crowds and parties. Upending the lives of these social animals have no bearing at all on how this pandemic is addressed. If they take a reality check, they will realize that when the dust settles, unlike the 80% of the lower socioeconomic working class, they will be back to their spoiled, privileged daily lives sipping designer coffees and hanging out at bars or other forms of reckless or blissful living. Their whining is annoying. Someone should slap them to reality.
Finally, there are the opportunists who take advantage of the gullible and/or the vulnerable. Those heartless businessmen who hoard medical supplies and sell them at extravagant prices, or peddle equipments, tools, medicines, medical devices that have no scientific value or at best useless for diagnosing or treating COVID-19 should be punished for economic sabotage. Sadly, some of them have direct connections with government officials who are accomplices to criminal acts of deception. The vermins who take advantage of a crisis for personal economic gain and thrive on disasters for financial remuneration will have their comeuppance.
Growing up in the metro, I remember seeing only deserted streets during the Holy Week, especially Good Friday. That’s the best day of the year for me. When the daily rush of work is placed to a one day pause, it’s a wonderful feeling to breath for a day. The past few days has been a quiet one. One of solitude and peace. It has allowed me (and hopefully all of us) to reflect on life at a time of a pandemic.
As each day evolves, we get to see the good in humanity. Those selfless people who give more of themselves than you would expect. The extraordinary heroes during unprecedented times. Those who think out of the box in order to share our Filipino bayanihan spirit. Not having to think about what we can do about ourselves, but sharing whatever we can and have because we care more about our neighbors. Symbolically, the season of lent did not come at a better time to symbolize the strength, resiliency and sacrifice during this time of crisis.
Then there are the wolves. I am lost for words at describing the decrepit people who walk among us. They will forever be a symbol of evil lurking among good. They will remind us that the battle of the novel coronavirus is not between science and the virus, but a representation of the fight between good and evil. The struggle is real but that should remind us that in both good and bad times, we will survive this.
Sit back. Breath. Appreciate your family and friends. Enjoy the new found freedom from the humdrum of work. Go for a walk. Listen to music. Finish a book. Binge on Netflix. Break up with your boyfriend or girlfriend. Connect with yourself and sit down and contemplate on the life you’ve really wanted.
There are a million things you can do. And should do. Those things and tasks you’ve sidelined can be addressed now.
Perhaps the coronavirus outbreak is a gentle reminder to us that life will show its beautiful side in the midst of being ugly. That life is fleeting. That life is a gift and should be celebrated. Everything else that happens around us is just a bonus or noise.
So yeah. Coronavirus and all its relatives will go down in science and history as one of mankind’s greatest adversary.
Over a decade, it has caused deadly diseases -SARS (severe acute respiratory syndrome) and MERS-COV (Middle East respiratory disease from coronavirus). Now, its cousin called COVID19 is spewing another flu-like disease that’s causing disproportionate global panic, confusion and havoc. Unlike its earlier cousins SARS and MERS which have more severe outcomes, the chaos generated by COVID19 is taking a greater toll on health, travel, business, and the global economy. It has upended the “way of life” in the 21st century.
SOCIAL MEDIA PLATFORMS AND QUACKS
In an era where social media and influencers dictate what is shared, liked or believable, the gullible are taking the war to a new level. The pandemic of infodemic is real. From conspiracy stories about the virus being manmade to a bioterrorist nightmare, pseudo-experts are frantically banging on their keyboards dishing out “opinions” not in their field of expertise. Their objectives are unclear. Perhaps one borne out of the need for attention and a shot, albeit a temporary one, at popularity? The age of being technologically connected knows no boundaries. For sure, someone will always add hysteria in order to twist a story. Consternation and a sense for foreboding, after all, will always be a bestseller.
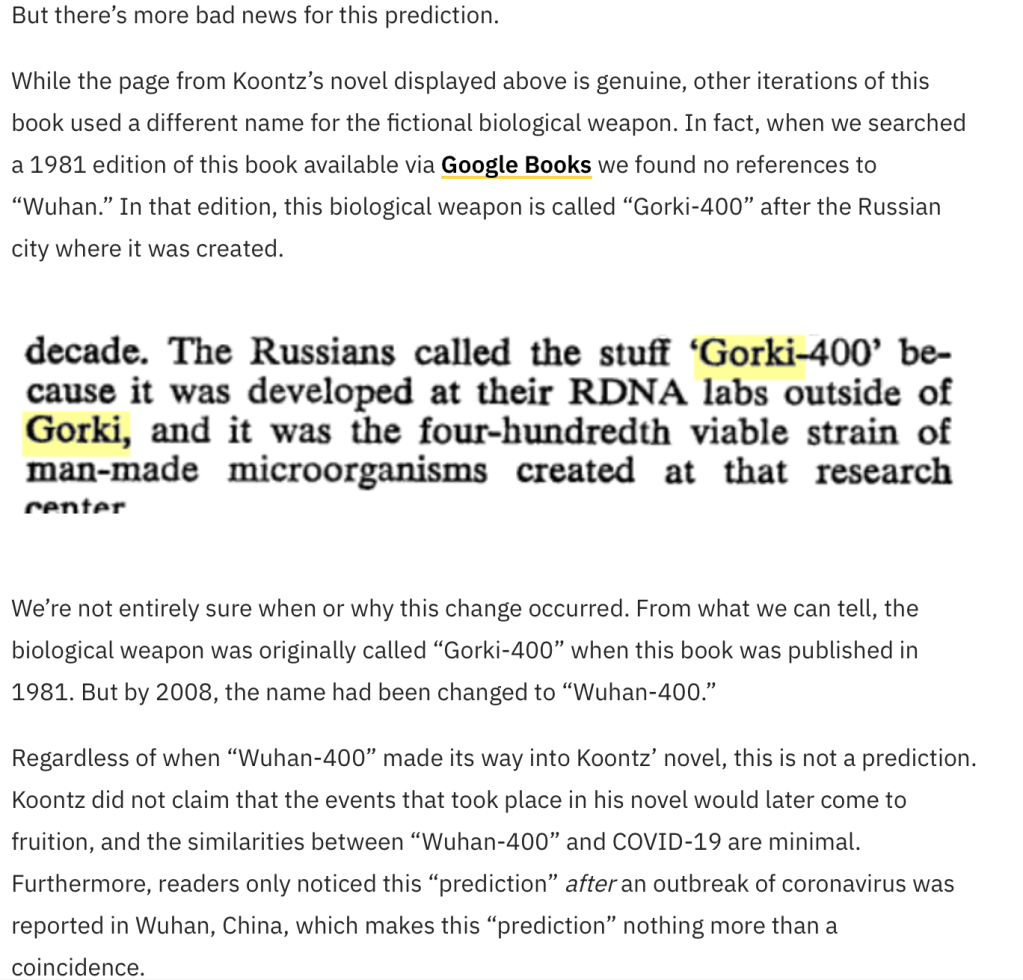
There’s a fictional book by Dean Koontz, “The Eyes of Darkness”, published in 1981 that refers to supposedly Wuhan-400 as a bioterrorism weapon in the city of Wuhan and predicting that in 2020, a severe pneumonia-like illness will spread throughout the globe and will suddenly disappear and return. This reference in a Nostradamus-like novel has been alluded to as well.
But this is where it gets weird. I don’t know if people actually know that the original book did not refer to this as Wuhan-400 but as Gorki-400. Let’s look at snopes.com and how they unravel the fake in this spread.
The animals that thrive in this infodemic spectrum are what I call the opportunists. They’re the kind of critters that spread “false” information on preventive measures and cures – peddling megadoses of multivitamins to devouring bushels of garlic and onions in order to apparently strengthen or insulate the immune system from viruses. With social media as a weapon, all the other propositions range anywhere from animal excrements to licensed drugs that are off label in use in the frantic search to place a stop to the outbreak. This act of desperation is human nature. We’re living in 2020 – a time of plenty, of travel, where social distancing is unheard of, where medical science is at its most advanced stage, and where miracles don’t happen anymore because we have an answer to every question. After all, it upended our normal day to day living in the 21st century.
The major difference between the influenza pandemic in 1918 and the infectious outbreaks of the 21st century is not only in the way the disease manifests itself. Social media platforms play a diverse, crucial and at the same time, deadly role in spreading either correct or wrong information. Suddenly, everyone is an expert – from the lowly troll keeper to the bored housewife to every Tom, Dick and Harry who is untrained and unable to discern with accuracy on what materials should be shared by Dr. Google. Search engines are churning out information that can simply be copied, pasted, shared, and the credulous person – like the coronavirus – simply spreads all these unverified data to the hapless ignoramus.
In the event of widespread illness, we’ll need to rely on accurate, vetted information to keep us safe. While the internet has made distribution easier than ever before, the democratization of information has created platforms and advertising economies built to reward misinformation.
Charlie Warzel, “Coronavirus will test our way of life” The New York Times, March 2, 2020
WHERE ARE WE NOW AND WHAT DO WE KNOW?
As the coronavirus seems to be getting a relief in Hubei in particular and China in general, the rest of the world is in highest alert as the numbers have spread outside of China and have amassed significantly in other parts of the world, particularly in Europe (where Italy is hardest hit).
The rapid global spread of the coronavirus has not only spread the disease but of racism and blame. Borders have been closed. Economies have been badly damaged. Governments have been criticized. Religion has bended back on traditional practice. One virus alone has brought the world to its knees. They say that the real human nature of a person is revealed during the worst of times. This is it.
What we now know is that the virus is being spread through local transmission with some people having no known contact or history of travel to China alone.
Like any viral respiratory disease (eg influenza), asymptomatic patients are difficult to identify. While adults and the elderly are at highest risk, children who have come in contact with family members who may be sick are not routinely being tested or isolated, or worst off, quarantined. “Super spreaders” can actually emanate from anyone who significantly move around sans conditional restraint. Daegu in South Korea was most affected because of a “super spreader” from a church group who continuously participated in activities and continued to proselytize in the community.
Like flu, COVID-19 presents with cough, colds, fever and other nonspecific symptoms. While they may be transmitted by similar routes, COVID-19 may be spread by the airborne route. We also know that the incubation period of COVID-19 seems to be much longer than influenza. The latter makes it more challenging to identify who are exposed and at risk. In addition, there are antiviral medications for the treatment of influenza and vaccine to prevent it. There is none for SARS-COV-2.
The varicella virus that causes chickenpox is a perfect example of a virus with a long incubation period. Patients are infective 3 days before and up to 5 days after the rashes appear. Meaning if your child has not had chickenpox and gets exposed to a classmate diagnosed yesterday to have the disease because the parents noted rashes only yesterday, most likely your child has been infected because the most infective period are 3 days prior to appearance of the rash up to 5 days after all the rash/vesicles have appeared. Because of the long incubation period, your child will most likely have chicken pox in the next 2-3 weeks.
QUO VADIS CORONAVIRUS?
Social distancing, isolation, quarantine, cancelled events and flights, lockdowns are interventions and measures used to control outbreaks in infectious diseases, particularly for those where we still have no treatment and no answers to more questions. YET.
What’s upsetting and causing the panic and hysteria is that as a people, we cannot accept the fact that in the past three months since the spread of this virus, it has finally landed home. Personal lives are now affected. In short, we simply cannot accept that there are just some things that we will need to give up for awhile while the medical community finds a solution as to how we can approach this novel respiratory virus with the limited resources we have.
Banging on the keyboards and instigating fear and worry is not helping anyone. It’s not like this is an easy puzzle to solve. You don’t know how much effort doctors and scientists are putting into this outbreak. How many of us are risking our own lives by attending to and pacifying a lynch mob who are desperate to get their lives back to what they used to be. We too, have our families who will grieve when we are gone. But we do what we do because we’re the only miracle workers left during times like these.
We are all on the same boat. Let’s not tilt too much on one side because it will sink if we do. Sit back. Relax. The waves will eventually die down. And if we all work together at addressing the problem in a calm manner, we will not overwhelm the limited health system. Overwhelming the current health care system affects efficiency and outcome of the critically ill and those who will require intensive care more than others.
Let’s try to be more socially and morally responsible in the kind of information that we share because the same shared spaces on social media with friends and family are multiply contagious as well.
I was telling a few friends the other day that if there is one Tagalog word that best describes the Filipino, it is the word “BASTA“.
It’s an apt description where the person thinks of himself and when cornered for an answer as to why they do what they do, the answer is BASTA.
It would help if we shoved that up our pride filled ass for awhile. This is not the time to care less. Only then can things get better…
“Sometimes the wrong train takes you to the right station”
– an Indian proverb
It’s not often that a Korean telenovela sweeps me off my feet. While most of the shows have original stories and screenplays and exceptional technical work, their predictable endings usually leaves one miserably uncomfortable in the end. On prodding by netizens, and the recent win of “Parasite” as Best Picture at the Oscars (yes, I loved the movie), I needed to see for myself what the buzz was all about over “Crash Landing On You”. After all, even Netflix had been “suggesting” I watch this series as well. [They weren’t wrong when I was overwhelmed at how good the story writings of Sky Castle and Hotel de Luna were.]
CrashLanding On You is the new K drama series that has everyone talking about how good a telenovela this is. After all, it’s not just an ordinary love story. The series takes us into two nations divided by a border, and even living in the 21st century, a sociopolitical cultural gap. The storyline is so well-stitched together that it embraces fate and destiny in the most unusual cross starred lovers – a South Korean businesswoman (Se-ri played by Son Ye-Jin) and a North Korean soldier (Ri Jeong-Hyeok played by Hyun Bin).
It weaves a story of power. Greed. Friendship. Loneliness. Suffering. Corruption. Family. Deception. Grief. Of good triumphing over evil. Of dreams and aspirations. And while there is a hodgepodge of conundrums convoluted in the drama, the most important story of all, told a hundred times each episode was clearly that of love, forgiveness, goodbyes and moving on.
The North Korean angle was a bit confusing for those of us who are not from the two Koreas. We’re told of horror stories of North Korea and while it makes no mention of Kim Jong-Un, it tells of the rigid government of the country. The shuttle back and forth from Pyongyang (the capital of North Korea) and the small village that delineates the border of the Demilitarized Zone (DMZ) between South and North Korea is the central setting for the series. The north is more popularly known for an absolute authoritarian regime, where capital punishment is imposed on many crimes ranging from grand theft to defection, treason, espionage, among a few. Executions are carried out by firing squad or hanging in public. While the series provides us a sneak peak into the lives of North Koreans, such as the disparity in provisions of the higher military officials (from housing to cars), the kind of food that is available to the lower class people and the different degrees and extent of corruption, this angle was subtly hidden away. I couldn’t tell the difference in the accents of Koreans from the South and the North. But that’s because I was an outsider trying to figure out the English subtitle.
Interspersed between some light moments was heavy drama. Sometimes to the point of being impossible. Yet one cannot help but turn a blind eye to that impossibility that even in the movies, anything can happen. But I will leave that to the audience to judge as this is one series that I highly recommend and I won’t spoil it by telling you each episode.
The scenic settings in Korea, Mongolia and Iseltwald, Switzerland was breathtaking and gave justice to the theme of Crash Landingon You.
Then there’s the side story of another kind of love. Between Dan and Seung-Jun. The kind of love that would overcome one’s own destiny and altruism that parallels that of the stars of the show, but would end tragically sans regrets (and a bit of payback to boot).
Crash Landing On You
It’s difficult not to fall in love with the story. After all, the central theme of love and selfless giving revolved around each and every protagonist character in the series. Their darkest and brightest moments.
The most wistful of all is the conversation between Yoon Se-Ri and Ri Jyeong Hyeok where Se-Ri tells Jyeong Hyeok:
There’s an Indian proverb that goes…sometimes the wrong train takes you to the right station. It was like that for me too. Throughout my life, I always felt like I was on the wrong train. One time, I wanted to give up. I didn’t want to go anywhere. So I thought about jumping off the train. Look where I am now. I took the wrong train again, and a very wrong one at that. It even got me across the 38th parallel. Still, you should think about the future, even if things don’t always go as you wish. I wish you could stay happy even after I leave, Jyeong-Hyeok. I want you to arrive at the right station, no matter what train you take.
Those lines alone…they were worth the 16 episodes.
Hope and love will always be a beautiful landing on anyone. This is a series that will long be remembered…because we all hope to arrive at the right station in spite of the wrong train rides in life.
In just two days, the novel coronavirus was christened twice.
COVID-2019 is the official DISEASE name when you get sick with the 2019 novel coronavirus. The virus has a new name as well. It’s called SARS-CoV-2.
The Coronavirus Study Group (CSG) of the International Committee on Taxonomy of Viruses [Gorbalenya, A. “Severe acute respiratory syndrome-related coronavirus – The species and its viruses, a statement of the Coronavirus Study Group”, bioRxiv] had decided to call the virus, severe acute respiratory syndrome coronavirus 2, or SARS-CoV-2.
The naming issues between the World Health Organization and the Coronavirus Study Group had caused a bit of chaos on this matter. As reported in Science, here’s a run down on the name christening event:
Martin Enserink, ‘A bit chaotic.’ Christening of new coronavirus and its disease name create confusion, Feb 12, 2020, 2:40PM
Unfortunately, China is reportedly objectionable to the name provided by CSG as it resisted comparisons between the current crisis and the traumatic 2002-03 coronavirus epidemic. And why the two names emerged almost simultaneously is also shrouded in mystery.
For now, in layman’s terms, SARS-CoV-2 is the name of the virus that causes COVID-2019. And you can get infected with SARS-CoV-2 and be asymptomatic or not get sick at all. But when you do get sick, then you have COVID-2019. It’s like when you get infected with the influenza virus, you can get flu…or something to that effect. [Did we really need to get more confusing than this? Seriously, there are people in media who would pounce at the discombobulated scientists and organizational groups who are leading, or misleading, the confused keyboard warrior who’s desperately trying to get a grasp of all this confusion.]
It’s not as if the “whats-in-a-name” has already caused confusion, health officials in China report more than 14,000 new cases in Hubei Province alone. The reason for the sudden surge in numbers? Changing the diagnostic criteria.
At the epicenter of the novel coronavirus outbreak are many people who are sick and yet have no access to being tested. The various hospitals in Wuhan (the largest city in Hubei Province) have been grappling on how to diagnose infections with “scarce and complicated tests that detect the virus’s genetic signature directly. Other countries, too, have had such issues.” [Roni Caryn Rabin, New York Times, 12 February 2020]
But the issue on the complicated tests and its waterloo wasn’t on China alone. On Wednesday (12 February 2020), the Center for Disease Control in the United States had announced that some of the “coronavirus testing kits sent to state laboratories around the country have flaws and do not work properly…But the failure of the kits means that states that encountered problems with the test should not use it, and would still have to depend on the CDCs central lab, which could cause several days’ delay in getting results.” [Denise Grady, New York Times, Updated 13 February 1:03am ET]
The sudden surge in cases is due to the government including now cases diagnosed in clinical settings including CT scan findings. “The change in reporting is meant to provide a more accurate view of the transmissibility of the virus. The new criteria is intended to give doctors broader discretion to diagnose patients, and more crucially, isolate patients to quickly treat them.”
Some government experts noted that the lack in testing kits in the provinces, its low accuracy of 30-40%, the slow turn around time for the test results, and the overstretched hospitals in the epicenter were enough reasons to look at the clinical diagnosis of the disease instead.
With so much at stake and muddling and befuddling this disease entity, this sudden shift in accounting has become an epidemiologists nightmare as well. How do you now accurately track the cases of SARS-CoV-2 as causing COVID-2019? Like so many diagnostic tests out there, the timing of when to actually take specimens matter. Patients may have no symptoms and yet turn out positive or other patients may be severely ill in the late stage of the infection and turn out negative.
When scientists, the medical community and governments are thrown at the epicenter of panic and chaos and become confused, providing accurate public information becomes a challenging task. Crisis management should always center on the patients who are afflicted.
The secret of crisis management is not good vs. bad. It’s preventing the bad from getting worse.