EVERYTHING GETS WORSE BEFORE IT GETS BETTER
So yeah. Coronavirus and all its relatives will go down in science and history as one of mankind’s greatest adversary.
Over a decade, it has caused deadly diseases -SARS (severe acute respiratory syndrome) and MERS-COV (Middle East respiratory disease from coronavirus). Now, its cousin called COVID19 is spewing another flu-like disease that’s causing disproportionate global panic, confusion and havoc. Unlike its earlier cousins SARS and MERS which have more severe outcomes, the chaos generated by COVID19 is taking a greater toll on health, travel, business, and the global economy. It has upended the “way of life” in the 21st century.
SOCIAL MEDIA PLATFORMS AND QUACKS
In an era where social media and influencers dictate what is shared, liked or believable, the gullible are taking the war to a new level. The pandemic of infodemic is real. From conspiracy stories about the virus being manmade to a bioterrorist nightmare, pseudo-experts are frantically banging on their keyboards dishing out “opinions” not in their field of expertise. Their objectives are unclear. Perhaps one borne out of the need for attention and a shot, albeit a temporary one, at popularity? The age of being technologically connected knows no boundaries. For sure, someone will always add hysteria in order to twist a story. Consternation and a sense for foreboding, after all, will always be a bestseller.
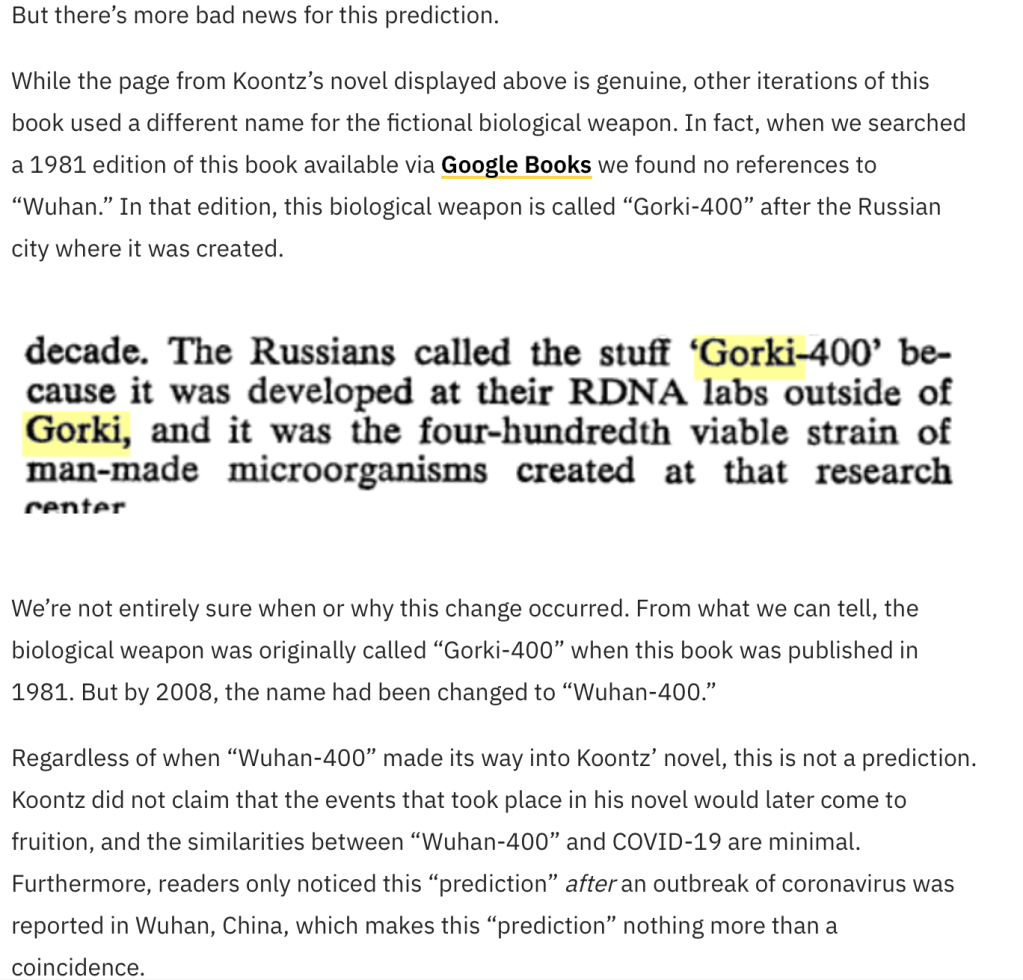
There’s a fictional book by Dean Koontz, “The Eyes of Darkness”, published in 1981 that refers to supposedly Wuhan-400 as a bioterrorism weapon in the city of Wuhan and predicting that in 2020, a severe pneumonia-like illness will spread throughout the globe and will suddenly disappear and return. This reference in a Nostradamus-like novel has been alluded to as well.
But this is where it gets weird. I don’t know if people actually know that the original book did not refer to this as Wuhan-400 but as Gorki-400. Let’s look at snopes.com and how they unravel the fake in this spread.


The animals that thrive in this infodemic spectrum are what I call the opportunists. They’re the kind of critters that spread “false” information on preventive measures and cures – peddling megadoses of multivitamins to devouring bushels of garlic and onions in order to apparently strengthen or insulate the immune system from viruses. With social media as a weapon, all the other propositions range anywhere from animal excrements to licensed drugs that are off label in use in the frantic search to place a stop to the outbreak. This act of desperation is human nature. We’re living in 2020 – a time of plenty, of travel, where social distancing is unheard of, where medical science is at its most advanced stage, and where miracles don’t happen anymore because we have an answer to every question. After all, it upended our normal day to day living in the 21st century.
The major difference between the influenza pandemic in 1918 and the infectious outbreaks of the 21st century is not only in the way the disease manifests itself. Social media platforms play a diverse, crucial and at the same time, deadly role in spreading either correct or wrong information. Suddenly, everyone is an expert – from the lowly troll keeper to the bored housewife to every Tom, Dick and Harry who is untrained and unable to discern with accuracy on what materials should be shared by Dr. Google. Search engines are churning out information that can simply be copied, pasted, shared, and the credulous person – like the coronavirus – simply spreads all these unverified data to the hapless ignoramus.
In the event of widespread illness, we’ll need to rely on accurate, vetted information to keep us safe. While the internet has made distribution easier than ever before, the democratization of information has created platforms and advertising economies built to reward misinformation.
Charlie Warzel, “Coronavirus will test our way of life” The New York Times, March 2, 2020
WHERE ARE WE NOW AND WHAT DO WE KNOW?
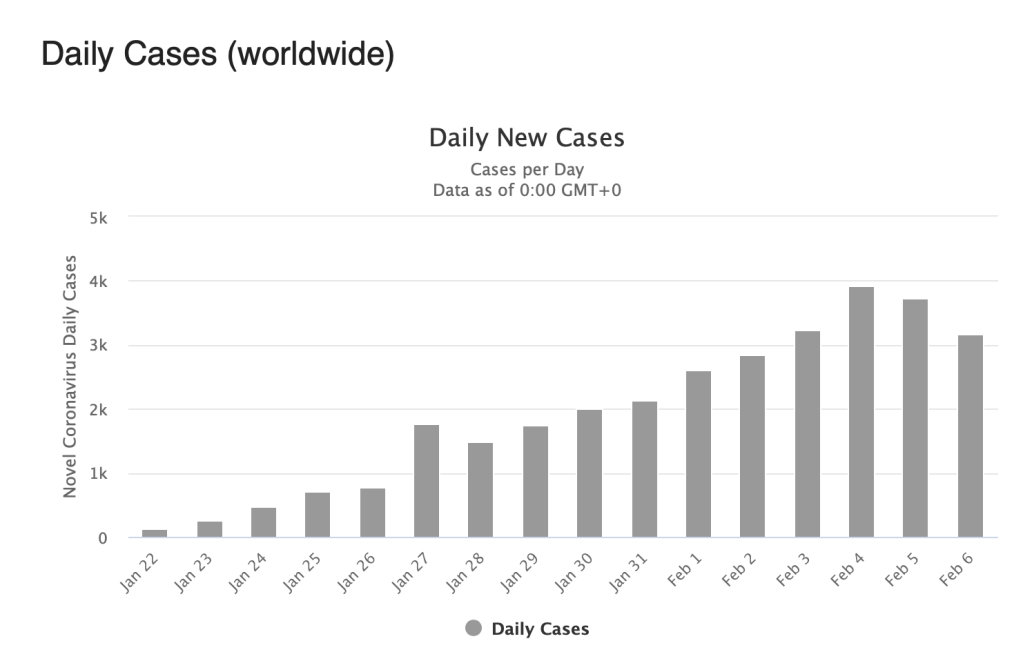
As the coronavirus seems to be getting a relief in Hubei in particular and China in general, the rest of the world is in highest alert as the numbers have spread outside of China and have amassed significantly in other parts of the world, particularly in Europe (where Italy is hardest hit).
The rapid global spread of the coronavirus has not only spread the disease but of racism and blame. Borders have been closed. Economies have been badly damaged. Governments have been criticized. Religion has bended back on traditional practice. One virus alone has brought the world to its knees. They say that the real human nature of a person is revealed during the worst of times. This is it.
What we now know is that the virus is being spread through local transmission with some people having no known contact or history of travel to China alone.

Like any viral respiratory disease (eg influenza), asymptomatic patients are difficult to identify. While adults and the elderly are at highest risk, children who have come in contact with family members who may be sick are not routinely being tested or isolated, or worst off, quarantined. “Super spreaders” can actually emanate from anyone who significantly move around sans conditional restraint. Daegu in South Korea was most affected because of a “super spreader” from a church group who continuously participated in activities and continued to proselytize in the community.
Like flu, COVID-19 presents with cough, colds, fever and other nonspecific symptoms. While they may be transmitted by similar routes, COVID-19 may be spread by the airborne route. We also know that the incubation period of COVID-19 seems to be much longer than influenza. The latter makes it more challenging to identify who are exposed and at risk. In addition, there are antiviral medications for the treatment of influenza and vaccine to prevent it. There is none for SARS-COV-2.
The varicella virus that causes chickenpox is a perfect example of a virus with a long incubation period. Patients are infective 3 days before and up to 5 days after the rashes appear. Meaning if your child has not had chickenpox and gets exposed to a classmate diagnosed yesterday to have the disease because the parents noted rashes only yesterday, most likely your child has been infected because the most infective period are 3 days prior to appearance of the rash up to 5 days after all the rash/vesicles have appeared. Because of the long incubation period, your child will most likely have chicken pox in the next 2-3 weeks.
QUO VADIS CORONAVIRUS?
Social distancing, isolation, quarantine, cancelled events and flights, lockdowns are interventions and measures used to control outbreaks in infectious diseases, particularly for those where we still have no treatment and no answers to more questions. YET.
What’s upsetting and causing the panic and hysteria is that as a people, we cannot accept the fact that in the past three months since the spread of this virus, it has finally landed home. Personal lives are now affected. In short, we simply cannot accept that there are just some things that we will need to give up for awhile while the medical community finds a solution as to how we can approach this novel respiratory virus with the limited resources we have.
Banging on the keyboards and instigating fear and worry is not helping anyone. It’s not like this is an easy puzzle to solve. You don’t know how much effort doctors and scientists are putting into this outbreak. How many of us are risking our own lives by attending to and pacifying a lynch mob who are desperate to get their lives back to what they used to be. We too, have our families who will grieve when we are gone. But we do what we do because we’re the only miracle workers left during times like these.
We are all on the same boat. Let’s not tilt too much on one side because it will sink if we do. Sit back. Relax. The waves will eventually die down. And if we all work together at addressing the problem in a calm manner, we will not overwhelm the limited health system. Overwhelming the current health care system affects efficiency and outcome of the critically ill and those who will require intensive care more than others.
Let’s try to be more socially and morally responsible in the kind of information that we share because the same shared spaces on social media with friends and family are multiply contagious as well.
I was telling a few friends the other day that if there is one Tagalog word that best describes the Filipino, it is the word “BASTA“.
It’s an apt description where the person thinks of himself and when cornered for an answer as to why they do what they do, the answer is BASTA.
It would help if we shoved that up our pride filled ass for awhile. This is not the time to care less. Only then can things get better…