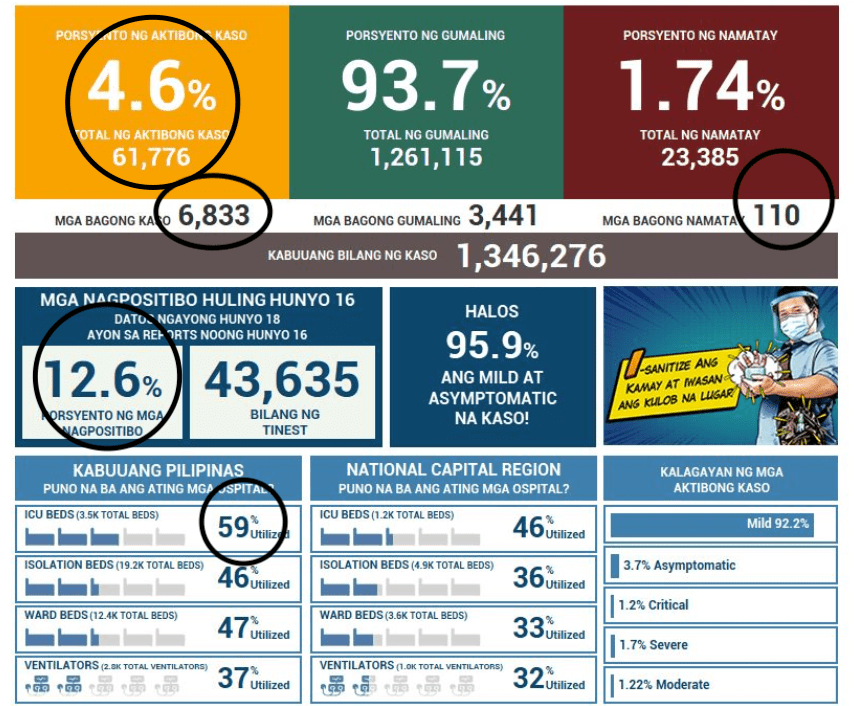
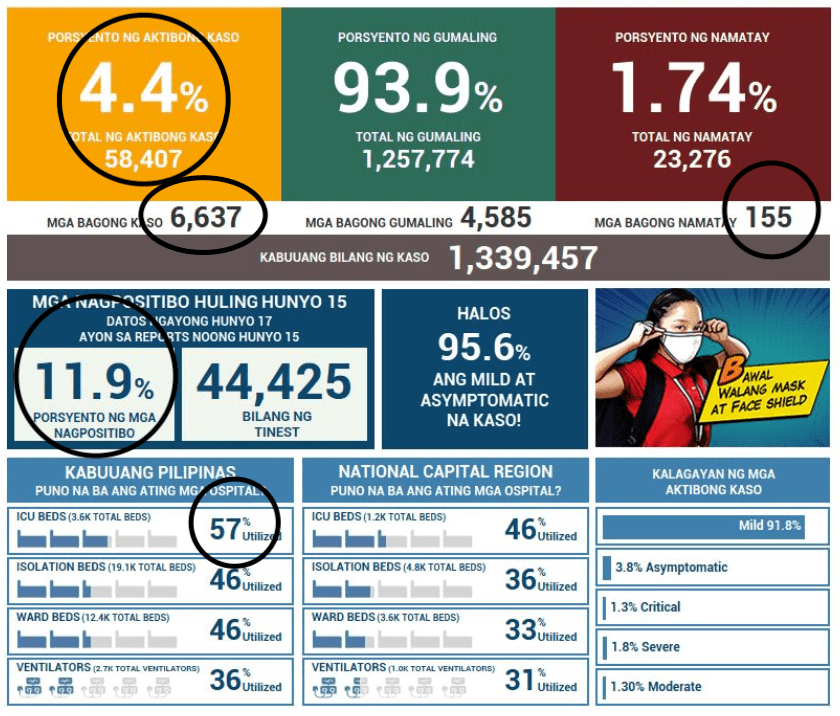
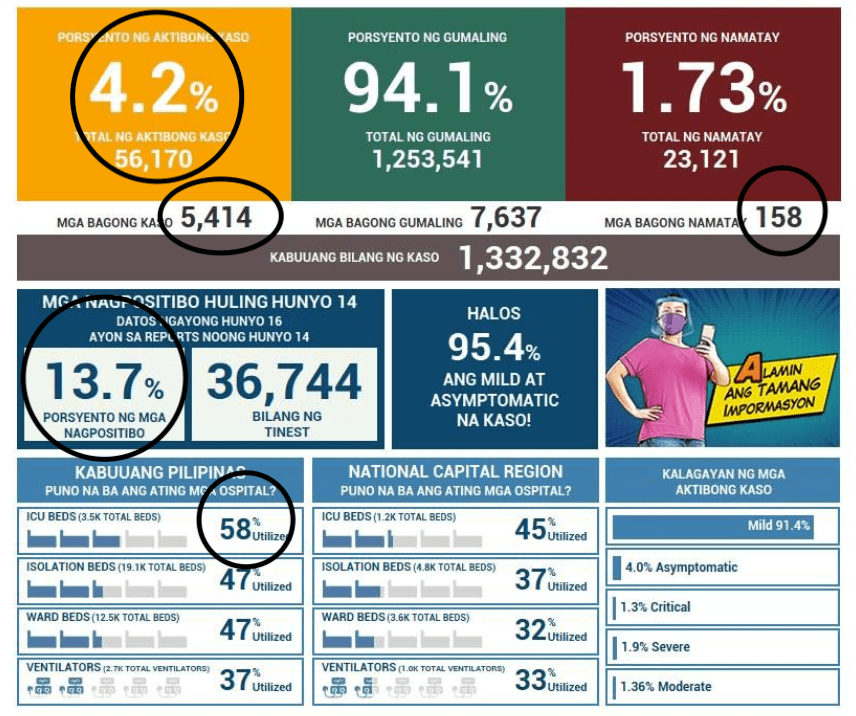
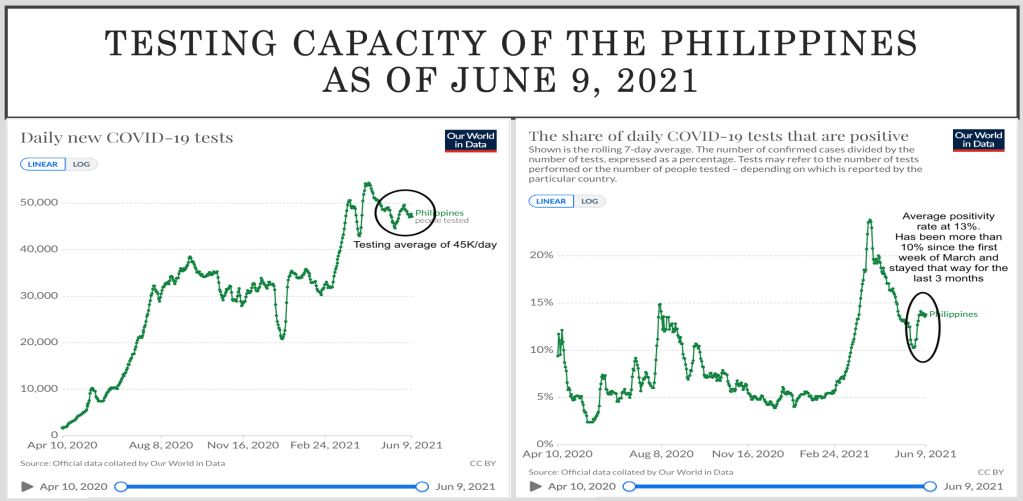
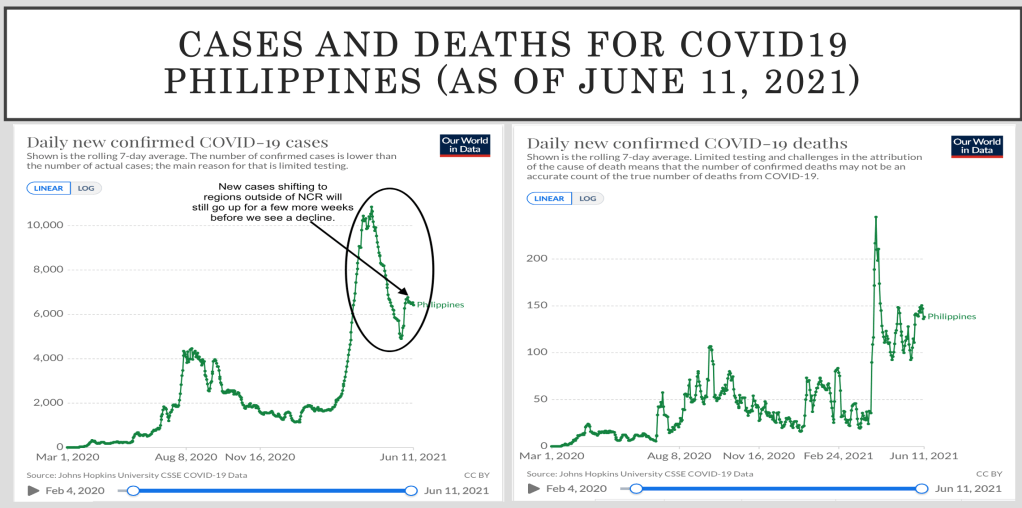
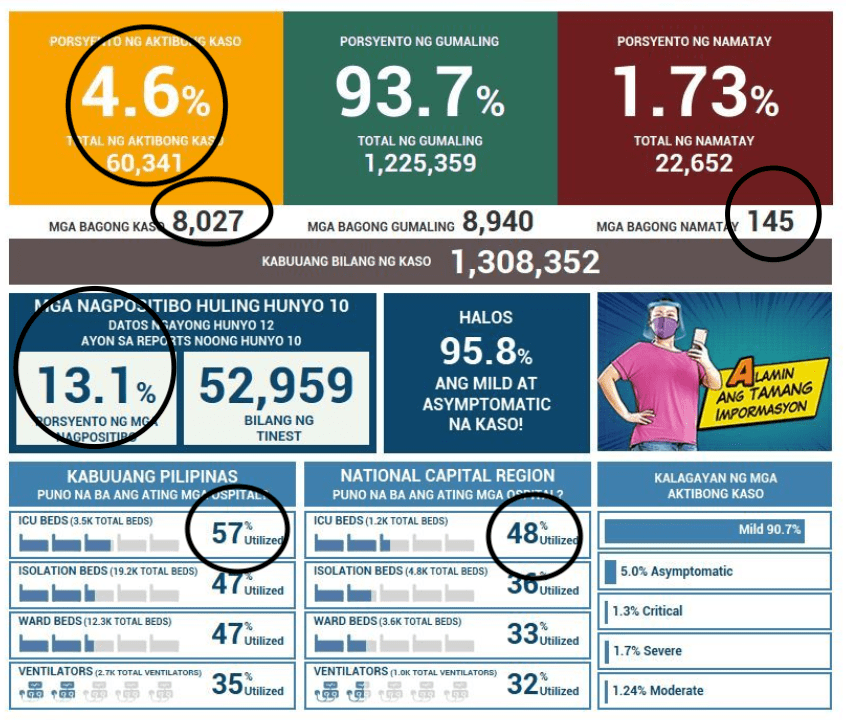
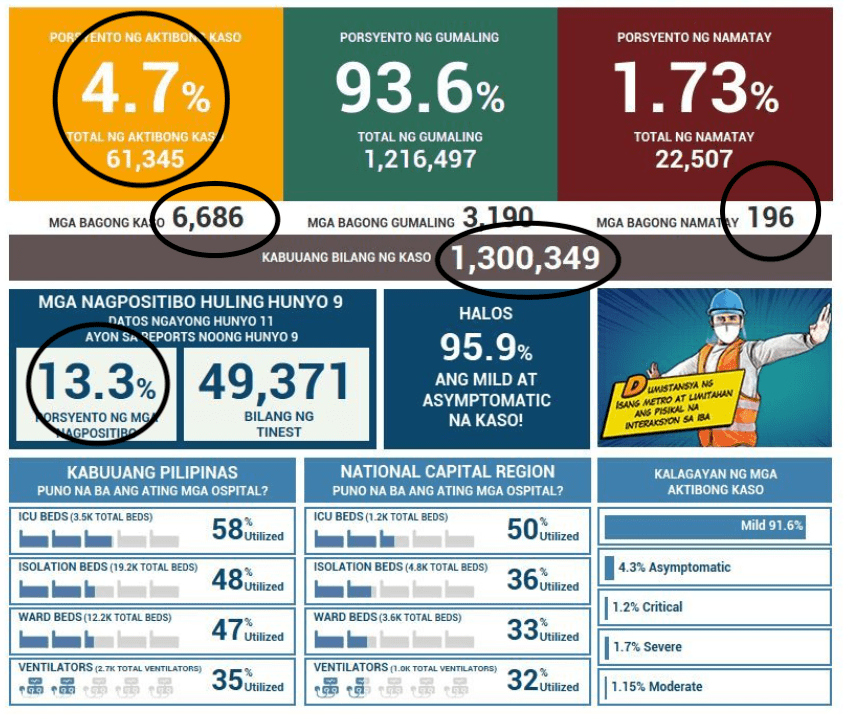
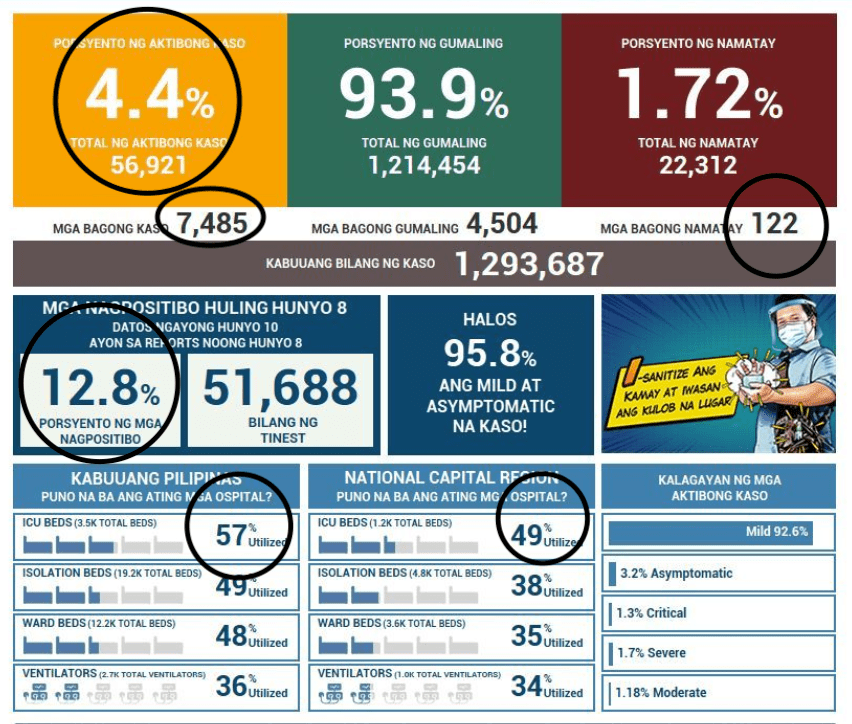
With 7,302 new cases today, from more than 50,000 tests done on June 11, with a positivity rate of 12.4%, the active cases remain close to 60,000. The over 8,000 cases yesterday was more than enough to take the Philippines back among the top ten countries with most cases in the world.
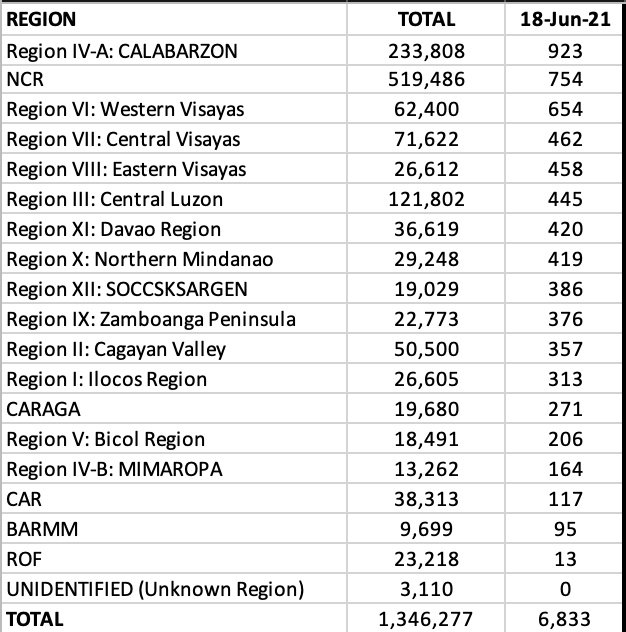
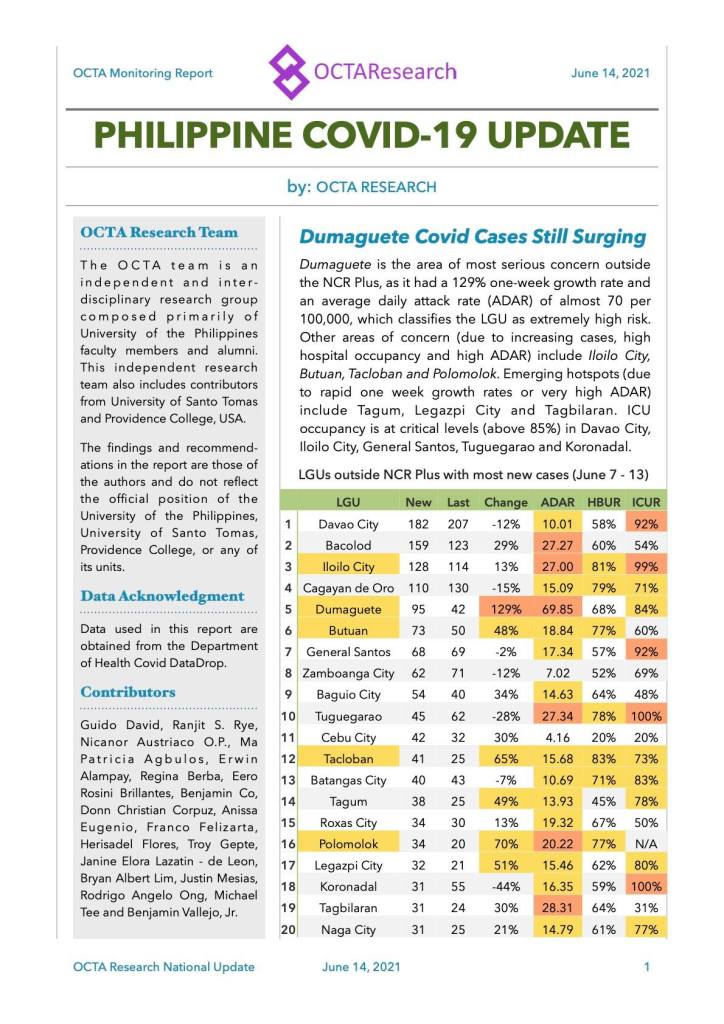
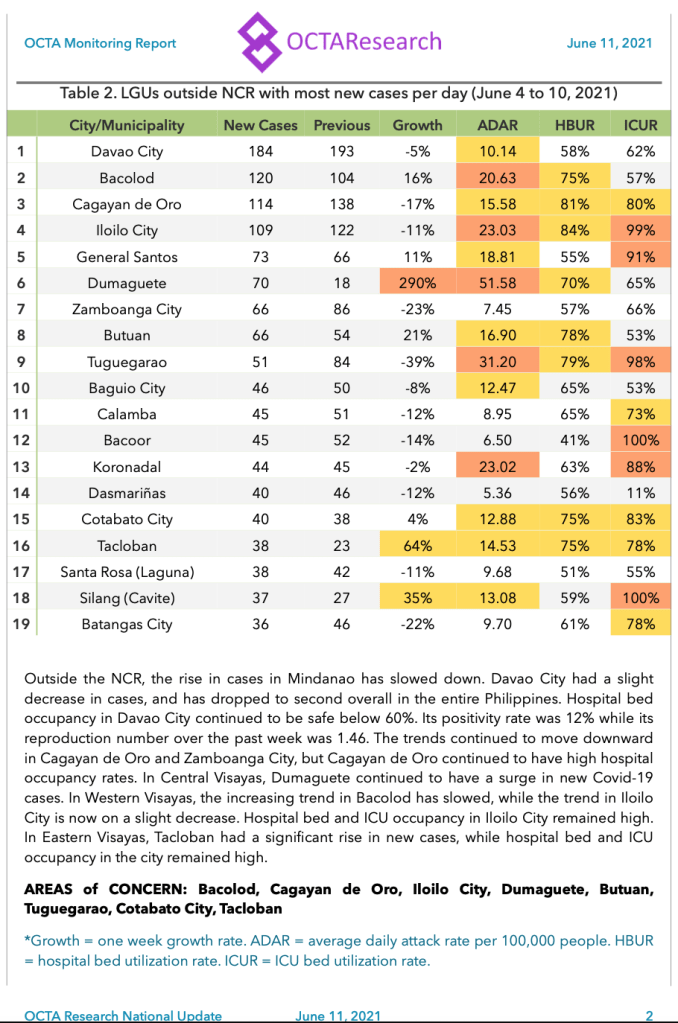
Cases in regions outside of the NCR are accounting for the higher number of daily cases and the healthcare and intensive care units in these areas significantly burdened.
With 137 new deaths reported today, the case fatality ratio for outcomes is at 1.81%.
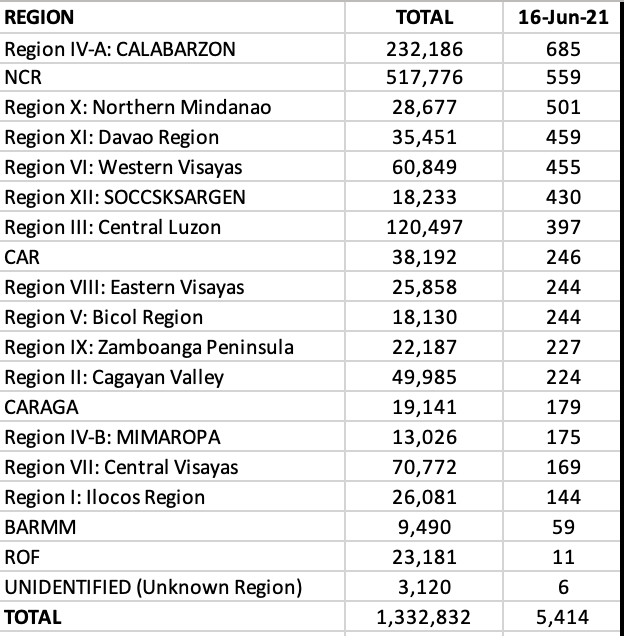
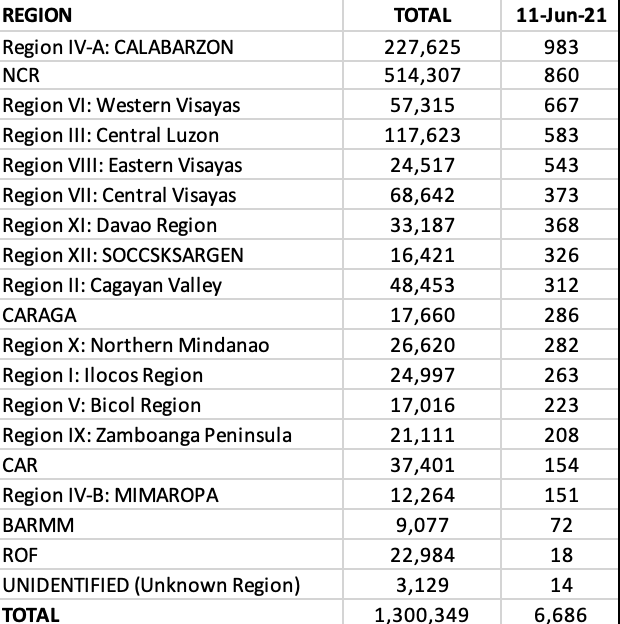
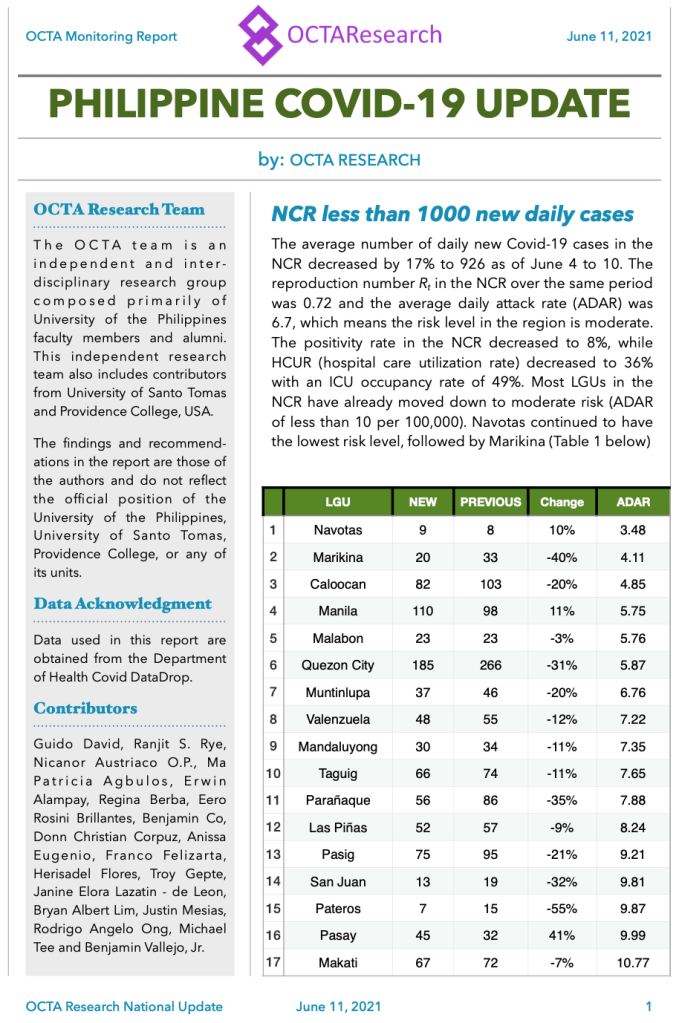
The National Capital Region moves a notch up to third, but remains behind CALABARZON and Western Visayas, and accounts for 11% of the daily total. Regions in Visayas and Mindanao continue to haul in cases for the day.
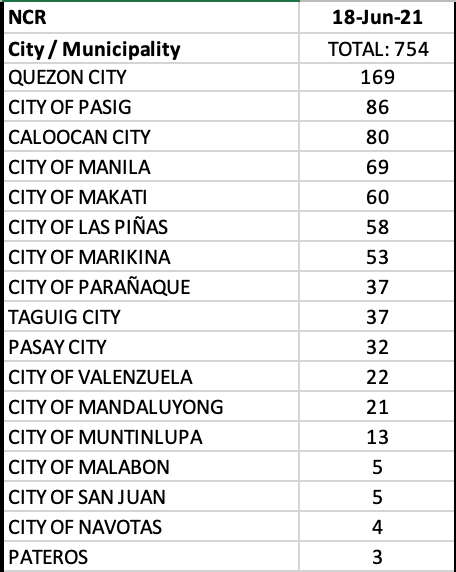
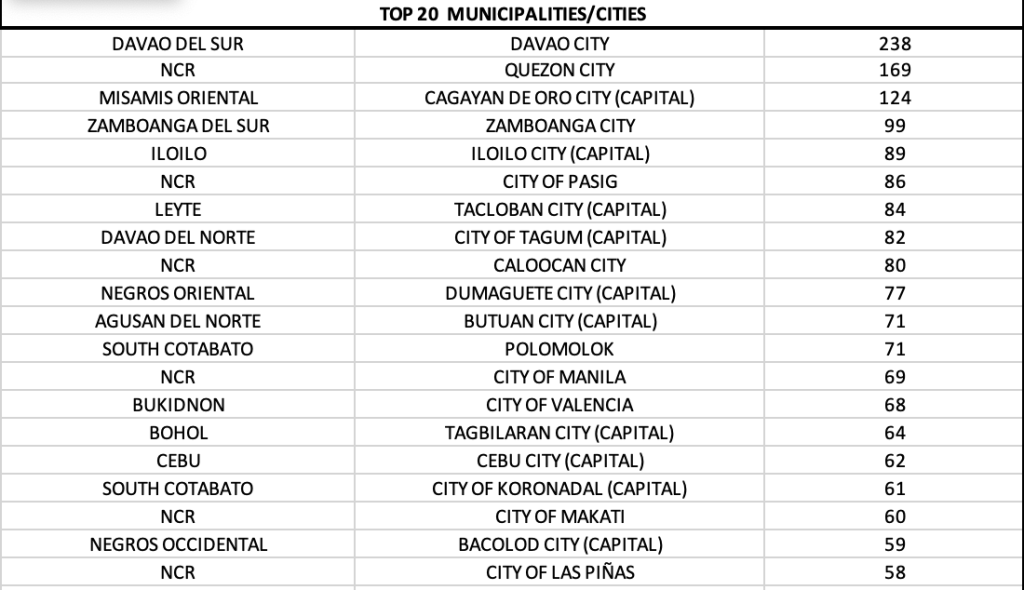
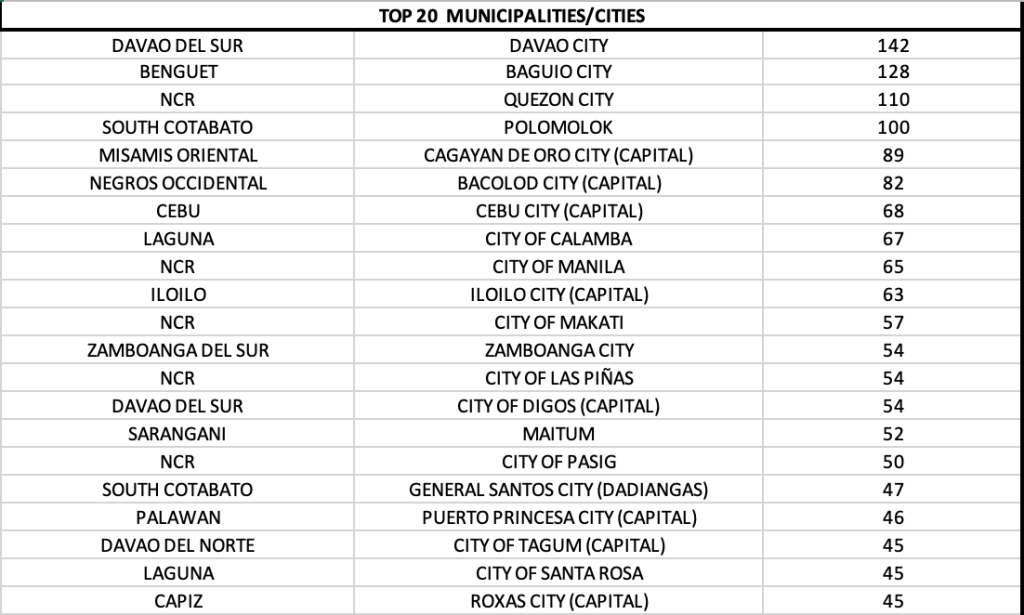
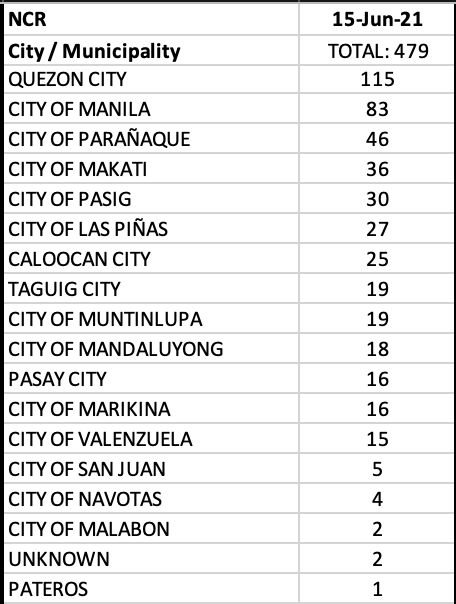
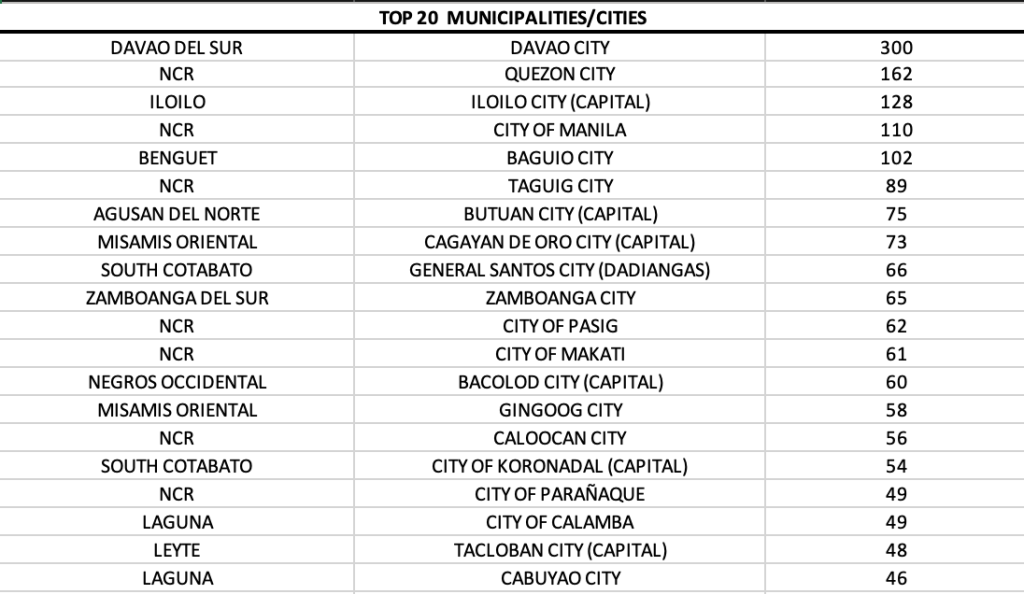
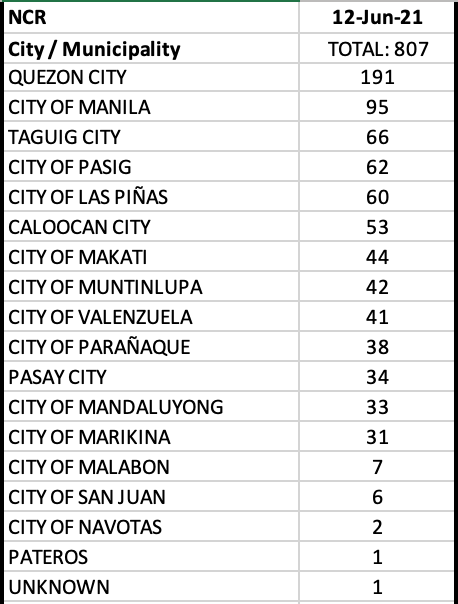
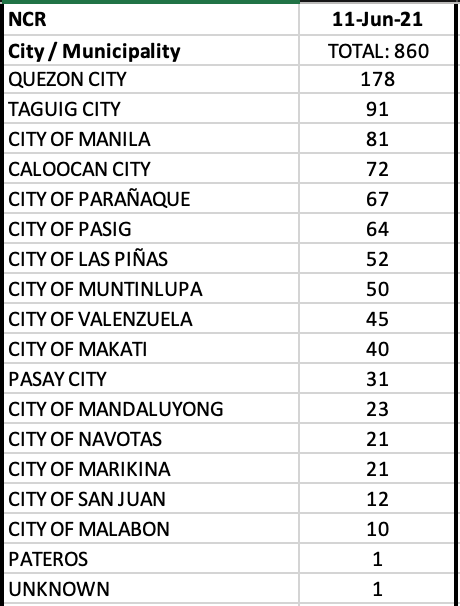
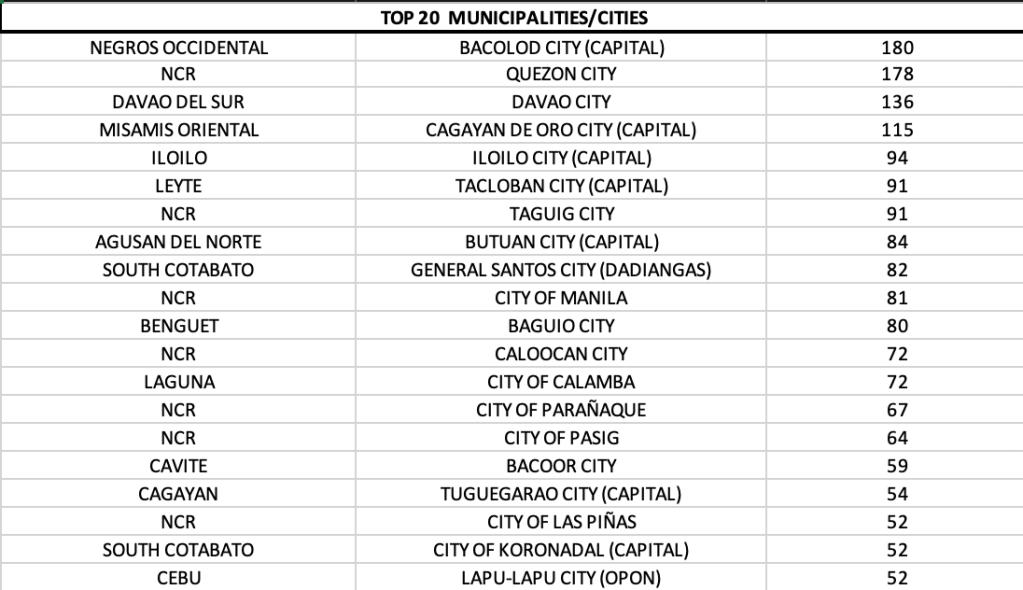
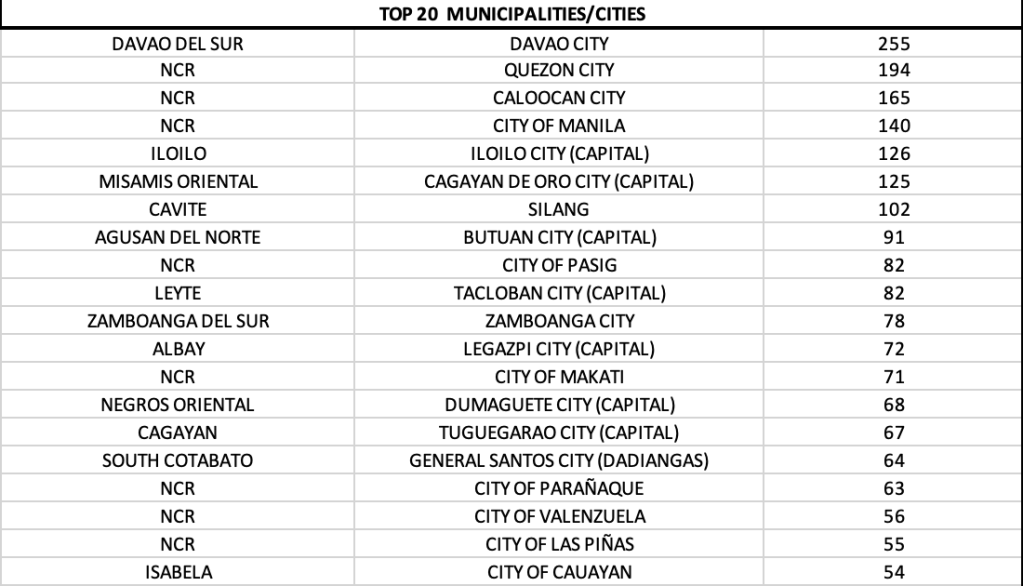
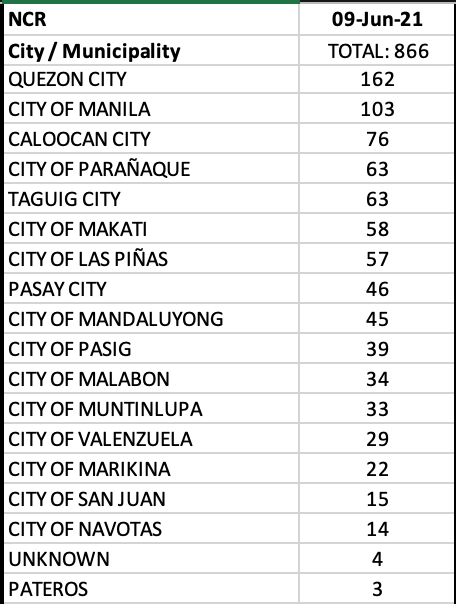
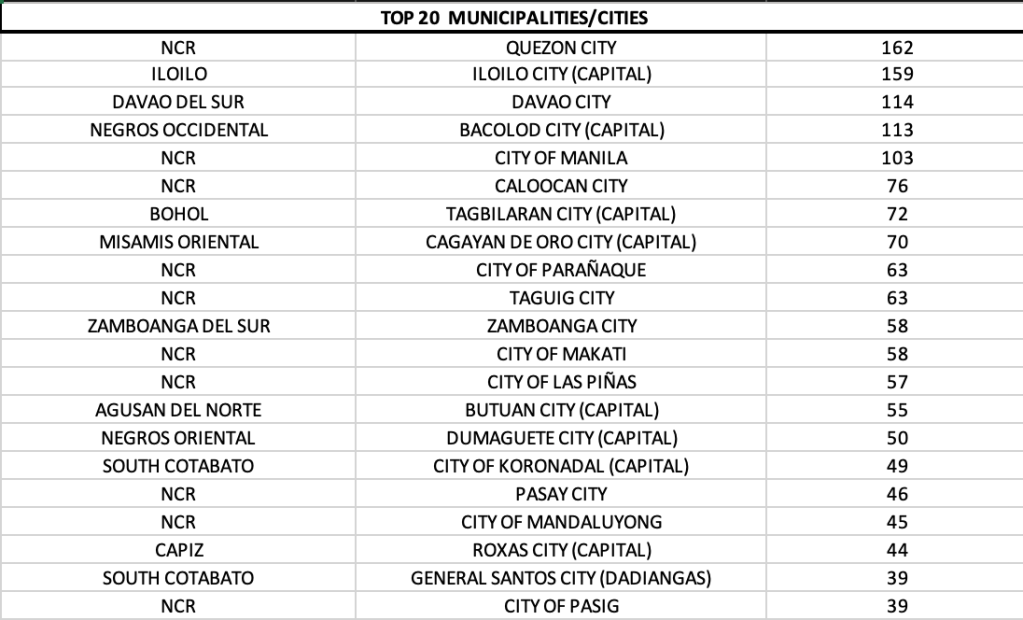
There were 7 of 17 LGUs in NCR that were in the top twenty cities/municipalities with most cases, with Quezon City and Manila leading the pack with triple digits.
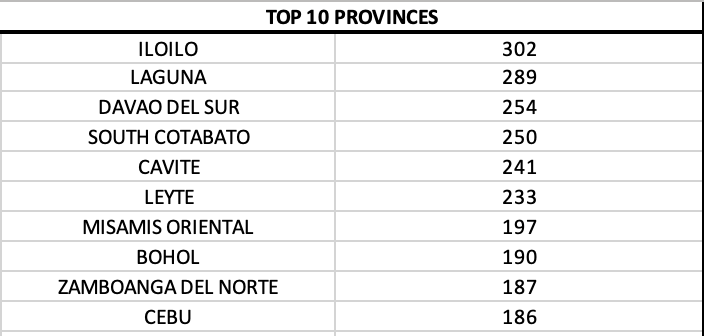
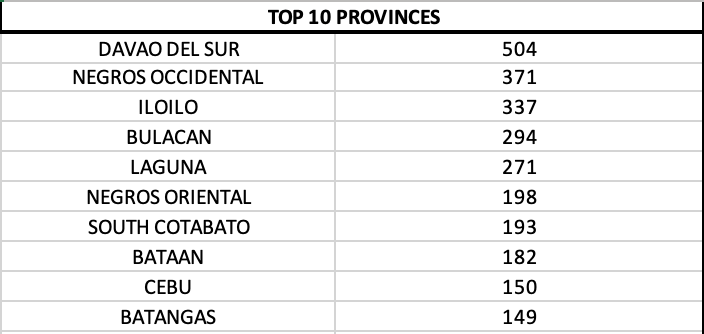
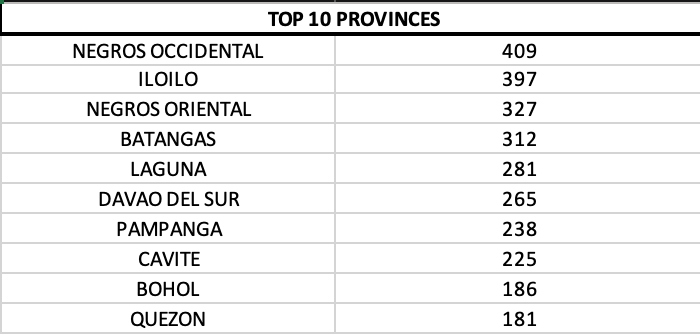
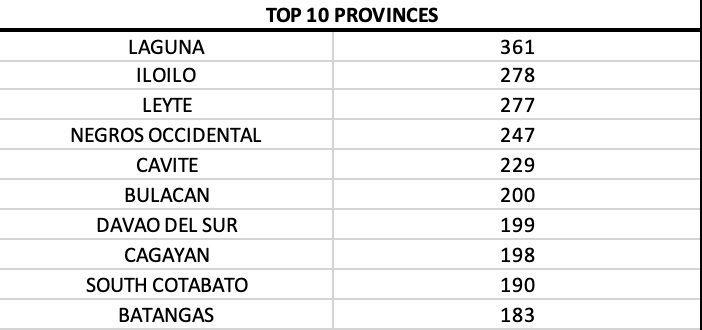
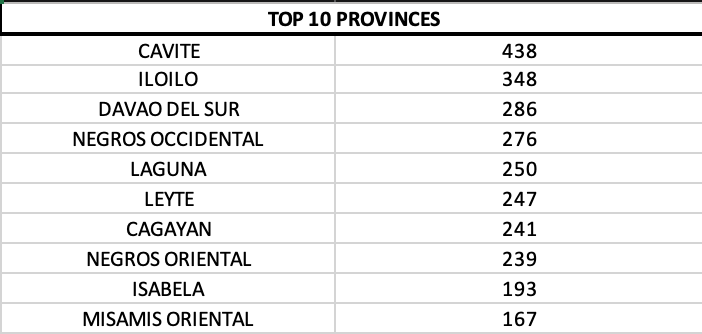
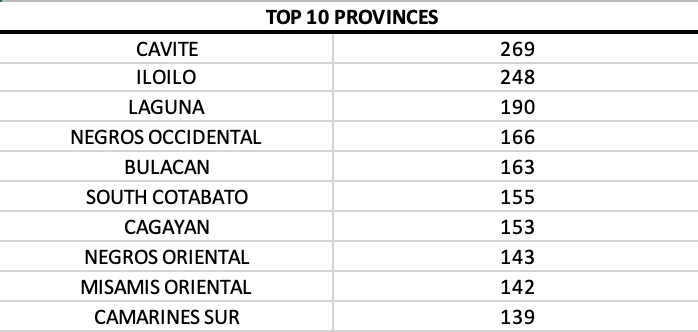
On a provincial level, Negros Oriental was in first spot for the first time. This was followed by provinces in Region VI – Negros Occidental and Iloilo.
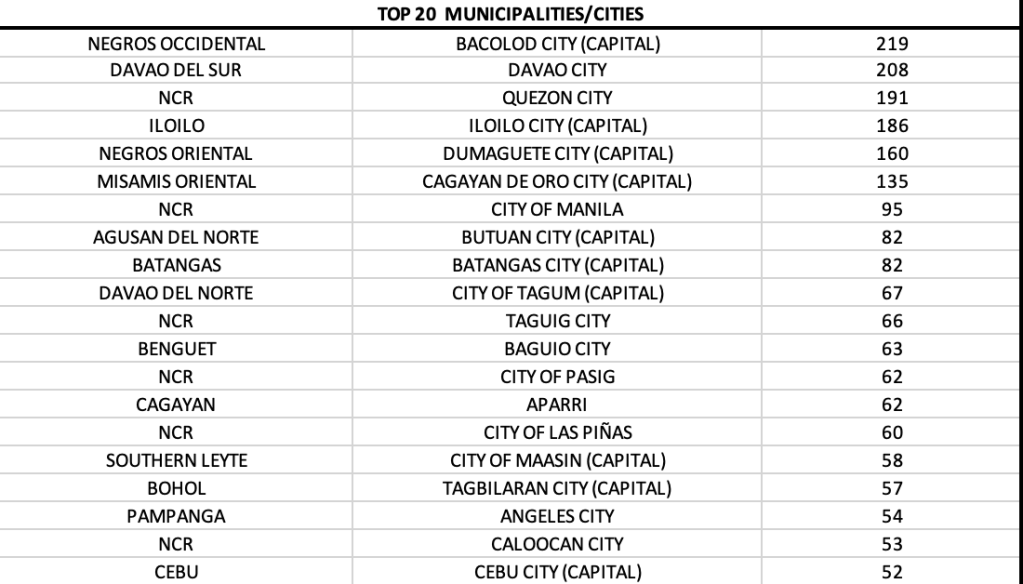
Quezon City was displaced to fifth over-all among cities with most cases in the country for the first time. The four cities that overtook it were from outside NCR – Bacolod, Davao City, Iloilo City and Dumaguete City. Surprisingly, Cebu City and Muntinlupa City are back in the top twenty cities with most cases today.
The week in review provides us an quick look at how the Philippines is faring compared to some of our Asian neighbors that also went through new surges and limited mobility measures. Unlike the Philippines, however, the mobility measures in other countries did not drastically affect their economies as there was no one size fits all rule. TTIQ (testing, tracing, isolation and quarantine) measures are standardized by the national government, and consistently implemented across all areas in their nation.
First is the hardy positivity rate. Based on the PH-DOH website, as of June 08, 2021, there are 260 accredited testing centers using rRT-PCR or cartridge-based PCR in the country https://doh.gov.ph/licensed-covid-19-testing-laboratories. However, 109 (42%) of these are all located in the National Capital Region. While NCR has the largest population per density (23,500 people per sq km), the imbalance in distribution of operational testing sites are more for economic rather than health policy reasons. For example, region III (Central Luzon) has 22, region IVA (CALABARZON) 21, region VII (Central Visayas) 20, and region XI (Davao Region) with 11 testing facilities.
The remaining regions have a sprinkling of testing facilities. Region IVB (MIMAROPA) has only 5 accredited testing sites – with 2 only for Palawan. The recent outbreak and rise in cases and positivity rate in Palawan is attributed to lack of testing. Region VIII (Eastern Visayas) that is seeing a dramatic increase in cases is also beset by lack of testing facilities with only 3 accredited sites – 2 located in Tacloban City and 1 in Ormoc City. The maldistribution of testing facilities in the regions outside of NCR leads to under testing and eventually, a high positivity rate.
Why does testing matter?
When people are not tested, we do not know who has COVID-19 infection. When people are not tested, it would be difficult to do contact tracing, and the infection just continues to spread. When people are not tested, isolation and quarantine cannot be done, and the disease sadly proliferates.
Second is the sudden shift in cases to the regions outside of NCR. As cases began to decline in mid-May, this decline did not last. As in the first surge, when the NCR had gone into stricter quarantine measures, many people in classes D and E needed to survive. The exodus back to their home provinces most likely accounted for the rise in cases in the regions. The second surge became more difficult because the hospitals not only filled up, overflowed, and resulted in a near catastrophic collapse of the health care in Mega Manila. As the second surge was deadlier, with cases tripling the cases of the first surge, another exodus, was inevitable.
With variants of concerns spreading in various regions, the porosity of our borders together with a drive to stimulate tourism became a triggering factor for the sudden upward shift of cases before it could even drop to levels less than 2,000 cases. Mobility was inevitable as the economy took a beating. Economy needed to be revved up because 2022 is election year.
How do you rev up an economy based on the science of lockdown measures?
While lockdowns help bring down cases significantly, it should be used cautiously and judiciously. It is a measure of last resort. If a government has a good TTIQ pillar in place, it will not need to resort to lockdown measures to address every surge. It is why data analysts do what they do. Following the data provides eyes for the government to see what is going on on the ground. When, why and how measures should be instituted and what economic activities should be allowed. Only a science driven policy should be used for deciding the level of lockdown measures.
Finally, there is the vaccination roll out.
In the figure below is a summary of the status of COVID-19 vaccinations in select Asian nations. The Philippines isn’t doing too bad, but it isn’t doing too good as well. That is because most of the vaccines we current receive are donations. The donations came in trickles, and the full purchases of the national government are coming in aliquots as well. Because of this, the vaccination drive could not be put into full gear and had to be appropriated to the more vulnerable population first, and the hardest hit region – the NCR – ahead.
To date, less than 1.5% of the total population in the Philippines has been fully immunized.
The target of herd protection, however, is a challenging one because of the diversity of vaccines the country received, is receiving, or has bought. As various COVID-19 vaccines vary in efficacy, so will the number of people that will need to get immunized to achieve herd protection. A vaccine with 50-60% over-all efficacy will most likely need 100% of the population immunized as against a vaccine with 95% efficacy, which may render herd protection when 70% of the population are vaccinated.
We need to remember that getting a single shot of the vaccine (for 2 dose vaccines) will not provide adequate protection. Yet. It will take two to four weeks after the second dose before any immunologic response can even be guaranteed. With the tepid vaccine rollout and the rollout in limited locations because of inadequate supplies for now, caution and appropriate science based strategies should be taken when reopening the economy.
Finally, here is where we stand together with our next door Asian neighbors.
With today’s numbers, will the Philippines land again among the top ten nations with most cases in the world in tomorrow’s daily tally?